
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.191(1); 2019 Jan 7

Social and medical models of disability and mental health: evolution and renewal
Over the last 6 decades, many published commentaries, from both within and outside the medical community, have criticized medicine’s characterization and management of mental illness and disability. These critiques have often referenced the “medical model,” a term that has multiple meanings but has almost always been used pejoratively. Prominent critics have included disability scholars and self-advocates, who attacked the so-called “medical model” and espoused an alternative “social model,” which characterizes disability as the product of an unaccommodating and oppressive society, rather than an individual and medical problem.
The terms “social model” and “medical model” have frequently been used to highlight opposing views of disability, but there has been little historical examination of their origins and evolving meanings. 1 As a result, clinicians have had limited access to information about what these concepts mean to patients, making it difficult to respond adequately to the concerns they raise. For physicians, fully embracing social-model views would require political engagement and a greater focus on societal, rather than individual, problems. Even if most physicians do not adopt these roles, increased awareness of disability perspectives and familiarity with critiques of the medical model may help them to identify new ways of improving care for their patients, while also enhancing opportunities and support for clinical trainees and colleagues with disabilities.
The critique of the medical model originated in the psychiatry literature and has taken various forms since psychiatrist Thomas Szasz coined it in the mid-1950s. 2 One version, an antireductionist view, lamented the tendency of medicine to reduce disease and disability down to physiochemical factors. This genre of criticism was popular among health professionals, who called for reforming medical practice to make clinicians more sensitive to the complex psychosocial aspects of health and illness.

Disability self-advocates rally in San Francisco, California, in 1973 for improved governmental and social supports, and an end to the oppression of people with disabilities. This image is reprinted with permission from Anthony Tusler, AboutDisability.
A second, exclusionist strain — initially espoused by Szasz — did not seek to reform medicine, but to exclude certain areas from medical oversight. Proponents of exclusionist views argued that medical intervention in specific realms — like mental health and disability — was stigmatizing or oppressive. Some suggested that these issues required societal reform, not individual treatment.
Most physicians have found antireductionist critiques of medicine to be more palatable than calls for exclusion, because antireductionist reforms do not question the fundamental value of medicine in treating individuals with mental illness and disability. One prominent proponent of an antireductionist perspective in the 1970s was psychiatrist George Engel. He took on the medical model, calling for a move away from reductive natural science approaches, in favour of an alternative “biopsychosocial model.” Engel distinguished his view from Szasz and other “exclusionists” (Engel’s term) by arguing that mental illness was a disease, and that its biological causes should not be dismissed. 3 At the same time, Engel suggested that medicine required a more nuanced view of disease, which included recognition of psychosocial issues along with physiochemistry. 4 Engel’s biopsychosocial model retained a dominant role for physicians, while calling on them to look beyond laboratory findings to consider a patient’s social environment.
Although Engel did not specifically address disability, his biopsychosocial model was widely influential among clinicians who specialized in this area. An antireductionist form of medical model critique was prominently presented in the World Health Organization’s classification of disability, published in 1980 (since updated: www.who.int/classifications/icf/en ). Similar arguments were also espoused in other health-related books from this period, including Genetic Disorders and Birth Defects in Families and Society (1984), which featured chapters on the medical, ethical and social aspects of disability, written by physicians, patient advocates and clergy. In these forums, physicians acknowledged critiques of the medical model and accepted outside advice on how to make medicine more sensitive to psychosocial aspects of disability. However, this was done without questioning the medical view of disability as a problem that could be clinically defined and treated.
Outside of medicine in the 1970s, clinical psychologists and sociologists — influenced by Szasz — took up and expanded exclusionist perspectives, applying this strain of medical model critique to mental illness, behaviour and intellectual disabilities. Clinical psychologist George Albee was a vocal critic of psychiatric approaches to mental health, which he argued inappropriately pathologized people’s “problems of living.” 5 Similarly, clinical psychologist Wolf Wolfensberger criticized the application of the medical model to intelligence and behaviour. Albee and Wolfensberger called for alternative approaches, which removed these issues from medical oversight and focused on reforming social institutions to be more supportive of individual differences. Unfortunately, both men’s views were met with derision by many of their medical colleagues, and their perspectives remained little known by physicians.
Sociologists Erving Goffman and Kenneth Irving Zola also adopted an exclusionist strain of medical model critique, highlighting the isolation, stigmatization and medicalization of deviant behaviour. 6 , 7 Zola also helped to adapt Szasz’s exclusionist view of mental illness to encourage new perspectives on physical disabilities as a social rather than a medical issue. In doing so, Zola — who identified as having a physical disability — contributed in the 1980s to the burgeoning American disability self-advocacy movement. 7
At the same time, British scholar Michael Oliver adopted an exclusionist strain of the medical model critique in his formulation of the social model of disability. 8 The social model argued that disability was a status imposed on people with various forms of impairment, and therefore that disability was a political, not a health, issue. Social model proponents held that the medical model viewed personal impairment as the sole cause of disability, making an individual’s body the appropriate target for intervention. Oliver argued that disability was distinct from impairment, and instead was the product of an unaccommodating society. From a social model perspective, medicine’s focus on treating impairment reified the widespread conception of disability as an individual tragedy, rather than the outcome of oppressive social perceptions and arrangements. One way to combat oppression, social model advocates suggested, was to exclude disability from medical oversight.
Of course, everyone occasionally requires medical care, and for people with certain disabilities — especially progressive, chronic or painful conditions — medical interventions may be necessary to maintain well-being and livelihood. 9 Although the social model was an empowering new perspective for many people with disabilities, some struggled with the implication that their disability was entirely the result of social oppression, because this seemed to suggest that their individual impairments should be ignored.
During the 1990s, feminist disability scholars and self-advocates, including Jenny Morris and Liz Crow, called for a “renewed social model of disability,” one that largely retained an exclusionist perspective, but acknowledged that even in a world without disability discrimination, impairment would have negative individual impacts. 10 Crow argued that the negative effects of impairment, like chronic pain, can on their own interfere with one’s social engagement, and may be beneficially mitigated by medical intervention. 10
Since the 1990s, proponents of the social model of disability have widely embraced the view that impairment and disability interact, and that the individual challenges of impairment should not be disregarded. Nonetheless, many disability self-advocates continue to express substantial distrust in the medical community and its approaches.
How then can physicians, as helping professionals, enhance their care and support for people with disabilities? One option is greater political engagement: promoting the view that disability should be seen as a valued form of human diversity, rather than an individual and tragic problem to be lamented and solved.
Many physicians may believe that their strengths for fomenting change would be best realized working with individuals in the clinic, rather than in the political arena; and indeed, there remains plenty of work to be done within the clinical professions. One key area is mentorship: teaching trainees about disability perspectives, and why many self-advocates have adopted and maintained an exclusionist form of medical model critique.
Another very important avenue is in recruiting and supporting people with disabilities to join and thrive in the clinical professions. 11 Physicians have an important role to play in recognizing the unique strengths and equal competency of people with disabilities as clinical professionals. Many of these qualified individuals have recounted being made to feel out of place in medical culture. Fundamental changes to medical training programs and institutions that normalize disability accommodations for students, residents, fellows and practitioners have yet to be made. 12
If physicians want to take an important step in the evolution and renewal of their profession, to show that medicine is more supportive and accepting than many people with disabilities have, understandably, come to believe, then embracing a much more nationally representative group of people with disabilities to become full participants and respected members of the clinical professions would be an important and welcomed start.
This article has been peer reviewed.
Disability Studies: Foundations & Key Concepts
This non-exhaustive reading list highlights some of the key debates and conceptual shifts in disability studies.

Disability studies emerged out of the disability civil rights movement in the late twentieth century. Early scholarship distinguishes the medical model of disability, which locates physical and mental impairments in individual bodies, from the social model, which understands the world as disabling people. The social model names both architectural and attitudinal barriers as the cause of disablement. Over the last few decades, the field has expanded to include individuals with a wide range of disabilities—not just physical conditions, but also mental and chronic ones.

This list, far from exhaustive, highlights some of the key debates and conceptual shifts in the field. In addition to showcasing disability studies’ interdisciplinary focus, the list traces the relationship between D.S. and other minority fields of study. At its broadest, disability studies encourages scholars to value disability as a form of cultural difference. As the sources below reveal, ability should not be the default when it comes to human worth.
Weekly Digest
Get your fix of JSTOR Daily’s best stories in your inbox each Thursday.
Privacy Policy Contact Us You may unsubscribe at any time by clicking on the provided link on any marketing message.
Asch, Adrienne. “Recognizing Death while Affirming Life: Can End of Life Reform Uphold a Disabled Person’s Interest in Continued Life?” The Hastings Center Report , 2005
Bioethics scholar Adrienne Asch is one of the first scholars to bring a disability studies approach to bioethics. This essay addresses U.S. policy regarding decisions for end-of-life treatment and, more broadly, it critiques discourse surrounding “quality of life.” Asch attacks the slogan “better off dead than disabled” by showing how disability does not necessarily diminish one’s life. Instead, she argues, healthcare practitioners should focus on forms of care that give disabled people independence. She also offers pragmatic suggestions for how caretakers can affirm the humanity of patients receiving end-of-life treatment.
Baynton, Douglas. “Slaves, Immigrants, and Suffragists: The Uses of Disability in Citizenship Debates.” PMLA , 2005
Douglas Baynton’s groundbreaking essay foregrounds disability in accounts of American history. He assesses three U.S. debates regarding citizenship: the civil rights movement, women’s suffrage, and immigration legislation. This essay considers how disability has been used as a justification for the oppression of marginalized populations. For example, slaves were said to become “crazy” if they were granted freedom. Women were often described as mentally incapable of receiving an education. And immigrants have been cast as disabled due to racial difference. Baynton explores how attending to disability in its own right (rather than as a symptom of misogyny or racism) enables an intersectional analysis.
Brueggemann, Brenda Jo, Rosemarie Garland-Thomson, Georgina Kleege. “What Her Body Taught (Or, Teaching about and with a Disability): A Conversation.” Feminist Studies , 2005
Written from the perspective of three female scholars with disabilities, this essay is one of the first pieces of scholarship to address the presence of disabled faculty in the classroom. Brueggemann, Garland-Thomson, and Kleege explore the tension between wanting their disabilities to be normalized, but also wanting them to be present in students’ minds. In addition to discussing the difficulty of disclosure in the classroom, they explore how educators might adopt different approaches to teaching to accommodate instructors’ disabilities.
Davis, Lennard. “Crips Strike Back: The Rise of Disability Studies.” American Literary History , 1999
This essay reviews three publications that address disability studies from a humanities-based perspective. While D.S. first emerged in the social sciences, Davis makes a case for the centrality of disability studies scholarship in literary studies. More broadly, he proposes that disability studies should no longer be considered a narrow or specialized field. It’s applicable to us all.
Donaldson, Elizabeth J. “The Corpus of the Madwoman: Toward a Feminist Disability Studies Theory of Embodiment and Mental Illness.” NWSA Journal , 2002
This essay takes up the figure of the madwoman in literature. Adopting a feminist disability studies approach, Donaldson critiques the way feminist scholars read madwomen as merely symptomatic of patriarchal oppression, which discounts the reality of mental disability. She is resistant to framing disability as a metaphor and advocates for readings that consider disability alongside questions of gender.
Erevelles, Nirmala. “Race.” Keywords for Disability Studies (2015)
This short essay gives an overview of the relationship between disability studies and critical race studies. Erevelles shows how disability has been aligned with race. However, analogizing race to disability (or saying, “disability is like race”) eliminates the specificity of both identity categories. She uses special education as an example because it is a site where racial segregation takes place on the premise of disability. By attending to disabled people of color, she argues that we can achieve a more nuanced analysis, which accounts for how social forces like poverty and involuntary institutionalization exacerbate different forms of social marginalization.
Garland-Thomson, Rosemarie. “Feminist Disability Studies.” Signs , 2005
In placing feminist studies and disability studies in conversation, Garland-Thomson argues that both fields work to de-naturalize assumptions about embodiment and social roles. Her essay explores a range of pressing social issues, including selective abortion, caretaking, and reproductive rights.
Ginsburg, Faye and Rayna Rapp. “Disability Worlds.” Annual Review of Anthropology , 2013
Ginsburg and Rapp call for a critical approach to disability in the field of anthropology. Bridging the gap between the medical and anthropological fields, they shift toward understanding impairment as both environmental and cultural. They also consider what ethnography can bring to questions of disability within anthropological study.
Hershey, Laura. “Disabled Women Organize Worldwide.” o ff our backs , 2003
Recounting events from the NGO Forum on Women in China (1995) and the International Leadership Forum for Women with Disabilities in Maryland (1996), disability activist Laura Hershey moves beyond Western definitions of disability to offer a global perspective. In addition to showing how disabled women are doubly discriminated against, Hershey outlines how gender can influence the international movement for disability rights. She also considers how issues like poverty and illiteracy speak to the feminist and disability movements.
James, Jennifer C. and Cynthia Wu. “Editors’ Introduction: Race, Ethnicity, Disability, and Literature: Intersections and Interventions.” MELUS , 2006
This essay brings ethnic studies into conversation with debates regarding disability representation. From the nineteenth-century freakshow to forced sterilization, people of color have been disproportionately disabled, and James and Wu call for an intersectional approach to these complex subjectivities.
Kleege, Georgina. “Blind Rage: An Open Letter to Helen Keller.” Southwest Review , 1998
In this more personal essay, Kleege interrogates Helen Keller’s status as a disability icon. Kleege critiques the way disability has been individualized, refuting both tragic and triumphant representations of impairment. In describing her experience navigating everyday life as a blind woman, Kleege attends to the realities of living in a world not made for disabled people.
Kudlick, Catherine. “Disability History: Why We Need Another ‘Other.’” The American Historical Review , 2003
In this groundbreaking essay, Kudlick moves to situate disability studies in historical scholarship. Reframing disability as valuable, she argues that a renewed attention to bodily and mental impairments can revise our accounts of nearly all events in history—from women’s rights to labor movements. Her essay offers a comprehensive overview of books and articles pertaining to disability history, and, more specifically, deaf history.
Linker, Beth. “On the Borderland of Medical and Disability History: A Survey of Both Fields.” Bulletin of the History of Medicine, 2013
This essay addresses why the history of medicine and disability studies fail to interact. Linker begins by critiquing disability studies’ resistance to medical discourse. She argues that certain disabled people, especially those who are living with chronic conditions, often rely heavily on medical care, which is why the “medical model” should not be so readily dismissed. In turn, while disability history is typically understood as different from medical history, especially in the U.S., Linker argues for a greater need for cross-disciplinary collaboration.
Linton, Simi. “Reassigning Meaning.” Claiming Disability: Knowledge and Identity , 1998
One of the most foundational essays in the field of disability studies, Linton outlines how language has been important to naming disability as a political rather than medical category. She also addresses the problem of “overcoming rhetoric,” which fails to address disabled people’s need for access.
McRuer, Robert. “Crip Eye for the Normate Guy: Queer Theory and the Discipling of Disability Studies.” PMLA , 2005
McRuer is one of the first scholars to assess the relationship between disability and queerness. In this essay, he analyzes how the popular show The Queer Eye for the Straight Guy normalizes the disabled body. While representations of queer life often resist disability, he argues that queer and disability studies share a resistance to normalization, which should be embraced in future scholarship and activism.
Price, Margaret. Mad at School: Rhetorics of Mental Disability and Academic Life . University of Michigan, 2011
Price offers one of the first substantive accounts of mental disability, which has come belatedly to studies of physical disability. She focuses on higher education as a site that stigmatizes mental disability in its focus on rationality, cohesion, and cognitive agility. Her book offers a range of suggestions, many of which are pedagogical, for how mental disability might revitalize academic life.
Siebers, Tobin. “Disability in Theory: From Social Constructionism to the New Realism of the Body.” American Literary History , 2001
Siebers critiques the social model of disability, arguing that it fails to account for the experience of individual bodies. His term “the new realism of the body” calls for an assessment of the bodily effects of disability, which often cannot be altered through environmental transformations alone.
Wendell, Susan. “Unhealthy Disabled: Treating Chronic Illness as Disabilities.” Hypatia , 2001
This article broadens the definition of disability to include individuals with chronic illnesses. While people in the disability community often distinguish themselves from people who are ill, not all disabled people, she observes, are healthy. Wendell questions some of the main assumptions in disability activism and scholarship regarding social justice and reform. Dismantling the environmental effects of disablement will not always eliminate a body’s suffering, she argues.
Williamson, Bess. “Access.” Keywords for Disability Studies (2015)
This short essay gives a comprehensive account of the history of access and why it is a key term in D.S. Williamson argues that paying attention to access turns our focus away from the individual, highlighting instead the disabling makeup of the social world. Although access is easy to define, Williamson notes that it is hard to implement in practice because disabled people have conflicting needs.
Editor’s Note: This list has been updated to include publication dates.
JSTOR is a digital library for scholars, researchers, and students. JSTOR Daily readers can access the original research behind our articles for free on JSTOR.
Get Our Newsletter
More stories.

Wild Saints and Holy Fools

Building Classroom Discussions around JSTOR Daily Syllabi

Scaffolding a Research Project with JSTOR

Making Implicit Racism
Recent posts.
- Aurorae and the Green of the Night Sky
- Heritage Bilinguals and the Second-Language Classroom
- IceCube Detector Confirms Deep-Space “Ghost Particle” Phenomenon
- The Uneven Costs of Cross-Country Connectivity
- How Two Rebel Physicists Changed Quantum Theory
Support JSTOR Daily
Sign up for our weekly newsletter.
An Essay on Modeling: The Social Model of Disability
- First Online: 01 January 2009
Cite this chapter

- Anita Silvers 3
Part of the book series: Philosophy and Medicine ((PHME,volume 104))
3484 Accesses
4 Citations
From its first exposition almost half a century ago, the social model of disability has been aimed at altering both theory and practice, bringing about profound changes in people’s understanding of disability, and in the daily lives of disabled people as well. The social model’s foil, and on some accounts its antithesis, is the medical model of disability. Both models treat disability as a locus of difficulties. While the medical model takes disability to be a problem requiring medical intervention—and as both the prerogative and the responsibility of medical professionals to fix—the social model understands disability as a political problem calling for corrective action by citizen activists who alter other people’s attitudes and reform the practices of the state. These two conceptualizations of disability have been treated as competitors, as if one must prevail over and eradicate the other in thinking about who disabled people are and what should be said and done in regard to them.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Compact, lightweight edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
- Durable hardcover edition
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Similar content being viewed by others

A New Human Rights Model of Disability

Disability Paradigm Shifts

Areheart, B. (2008). When disability isn’t “just right”: The entrenchment of the medical model and the Goldilocks dilemma. Indiana Law Journal , 83 , 181–232.
Google Scholar
Barton, L. (1989). Disability and dependence. Lewes: Faimer Press.
Bate, W. J. (1978). Samuel Johnson. New York: Harcourt Brace Jovanovich.
Bickenbach, J. (1993). Physical disability and social policy. Toronto: University of Toronto Press.
Boswell, J. (1934–1950). Life of Samuel Johnson (G. B. Hill, Eds.; Rev. L. F. Powell). Oxford: Clarendon Press.
Bynoe, I., Oliver, M., & Barnes, C. (Eds.). (1991). Equal rights and disabled people: The case for a new law . London: Institute of Public Policy Research.
Chevron USA, Inc. v. Echazabal. (2002). U.S. Supreme Court 00-1406.
Crow, L. (1996). Including all of our lives: Renewing the social model of disability. In J. Morris (Ed.), Encounters with strangers: Feminism and disability (pp. 206–222). London: Women’s Press.
Davis, L. (2002). Bending over backwards: Disability, dismodernism & other difficult positions . New York: NYU Press.
Finkelstein, V. (1980). Attitudes and disabled people . Geneva: World Health Organisation.
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity . New York: Simon & Schuster, Inc.
Grady, D. (1998). Studies of schizophrenia indicate psychotherapy. NY Times (Tuesday, January 20, B17).
Hunt, P. (Ed.). (1966). Stigma: The experience of disability . London: Geoffrey Chapman.
Morris, J. (1991). Pride against prejudice: Transforming attitudes to disability . London: The Women’s Press.
Morris, J. (2001). Impairment and disability: constructing an ethics of care that promotes human rights. Hypatia, 16 (4), 1–16.
Article Google Scholar
National Academies. (2007). Outdated policies are impediment for Americans with disabilities; Report recommends ways to remove barriers to care, assistive services . Available at http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=04242007
Oliver, M. (1983). Social work with disabled people . London: Macmillan.
Pendo, E. (2002). Disability, doctors and dollars: Distinguishing the three faces of reasonable accommodations. Disability, Doctors and Dollars, 35 U.C. Davis L. Rev. 1175, 1191.
Rovner, L. L. (2004). Disability, equality and identity. Disability, Equality, and Identity , 55 ALA. L. Rev. 1043.
Samaha, A. (2007). What good is the social model of disability ? 74 U CHI. L Rev. 1251, 1257. Working Paper 166, Public Law and Legal Theory Working Papers, University of Chicago Law School. Available at http://lawreview.uchicago.edu/issues/archive/v74/74_4/Samaha.pdf
Scully, J. L. (2008). Disability bioethics: Moral bodies, moral difference. Lanham, Maryland: Rowman and Littlefield.
Silvers, A. (1998). Formal justice. In A. Silvers, D. Wasserman, & M. Mahowald (Eds.), Disability, difference, discrimination: Perspectives on justice in bioethics and public policy (pp. 13–145) . Lanham, Maryland: Rowman and Littlefield.
Silvers, A. (2003). On the possibility and desirability of constructing a neutral conception of disability. Theoretical Medicine and Bioethics , 25 (6), 471–487.
Silvers, A. (2005, Winter). Protection or privilege? Reasonable accommodation, reverse discrimination, and the fair costs of repairing recognition for disabled people in the workforce. The Journal of Gender, Race and Justice: A Journal of the University of Iowa College of Law, 34 , 561–594.
Silvers, A. (2007). Predictive genetic testing: Congruence of disability insurers’ interests with the public interest. Journal of Law, Medicine and Ethics, 35 (2), 52–58.
Silvers, A., & Stein, M. (2002). Disability, equal protection, and the Supreme Court: Standing at the crossroads of progressive and retrogressive logic in constitutional classification , 35 U. Mich. J.L. Reform 81.
tenBroek, J. (1966). The right to live in the world: The disabled in the law of torts. California Law Review, 54 CAL. L. Rev. 841, 858).
Stone, D. (1984). The disabled state . Philadelphia: Temple University Press.
Thrale, H. (1984). Dr. Johnson by Mrs. Thrale: The “Anecdotes” Mrs. Piozzi in their original form (R. Ingrams, Ed.). London: Chatto and Windus.
Union of the Physically Impaired Against Segregation (UPIAS) and the Disability Alliance. (1978). Fundamental principles of disability. Available at http://www.leeds.ac.uk/disability-studies/archiveuk/UPIAS/fundamental%20principles.pdf
Wendell, S. (2001). Unhealthy disabled: Treating chronic illnesses as disabilities. Hypatia, 16 (4), 17–33.
Download references
Author information
Authors and affiliations.
Department of Philosophy, San Francisco State University, San Francisco, California, USA
Anita Silvers
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Anita Silvers .
Editor information
Editors and affiliations.
Dept. Philosophy, Rice University, S. Main Street 6100, Houston, 77005-1892, U.S.A.
D. Christopher Ralston
Justin Hubert Ho
Rights and permissions
Reprints and permissions
Copyright information
© 2009 Springer Science+Business Media B.V.
About this chapter
Silvers, A. (2009). An Essay on Modeling: The Social Model of Disability. In: Ralston, D., Ho, J. (eds) Philosophical Reflections on Disability. Philosophy and Medicine, vol 104. Springer, Dordrecht. https://doi.org/10.1007/978-90-481-2477-0_2
Download citation
DOI : https://doi.org/10.1007/978-90-481-2477-0_2
Published : 28 August 2009
Publisher Name : Springer, Dordrecht
Print ISBN : 978-90-481-2476-3
Online ISBN : 978-90-481-2477-0
eBook Packages : Humanities, Social Sciences and Law Social Sciences (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Social Model vs Medical Model of disability
The social model vs the medical model of disability.
Social model of disability
The social model of disability says that disability is caused by the way society is organised, rather than by a person’s impairment or difference. It looks at ways of removing barriers that restrict life choices for disabled people. When barriers are removed, disabled people can be independent and equal in society, with choice and control over their own lives.
Disabled people developed the social model of disability because the traditional medical model did not explain their personal experience of disability or help to develop more inclusive ways of living.
(An impairment is defined as the limitation of a person’s physical, mental or sensory function on a long-term basis.)
Changing attitudes to disabled people
Barriers are not just physical. Attitudes found in society, based on prejudice or stereotype (also called disablism ), also disable people from having equal opportunities to be part of society.
Medical model of disability
The social model of disability says that disability is caused by the way society is organised. The medical model of disability says people are disabled by their impairments or differences.
Under the medical model, these impairments or differences should be ‘fixed’ or changed by medical and other treatments, even when the impairment or difference does not cause pain or illness.
The medical model looks at what is ‘wrong’ with the person and not what the person needs. It creates low expectations and leads to people losing independence, choice and control in their own lives.
Social model of disability: some examples
- A wheelchair user wants to get into a building with a step at the entrance. Under a social model solution, a ramp would be added to the entrance so that the wheelchair user is free to go into the building immediately. Using the medical model, there are very few solutions to help wheelchair users to climb stairs, which excludes them from many essential and leisure activities.
- A teenager with a learning difficulty wants to work towards living independently in their own home but is unsure how to pay the rent. Under the social model, the person would be supported so that they are enabled to pay rent and live in their own home. Under a medical model, the young person might be expected to live in a communal home.
- A child with a visual impairment wants to read the latest best-selling book to chat about with their sighted friends. Under the medical model, there are very few solutions but a social model solution ensures full text audio-recordings are available when the book is first published. This means children with visual impairments can join in with cultural activities on an equal basis with everyone else.
University Library, University of Illinois at Urbana-Champaign

Disability Theory: Medical/Rehabilitative Model
- Medical/Rehabilitative Model
- Social/Independent Living Model
- Researching Disability Theory
Medical Model of Disability
The medical model of disability focuses on the medical aspects of a disability and seeks to "cure" a person of their disability so that they can return as closely as possible to a able-bodied state. In the past and even today, this is a common way that people think about disability. The problem is contained in the individual who has the disability instead of the problem being with the environment around them. A disability's solution is by medical professionals who can cure the effect of a disability with things like prosthetics, surgeries, and medications. The rehabilitative model is closely related to the medical model. It focuses on the belief that belief that if the person with a disability makes an effort and works with rehabilitative services, they can overcome their disability.
This model is criticized by many people who are disabled and disability studies researchers and advocate because of its narrow view of the full lives that people lead despite and because of their disability. Many people who are disabled feel that their disability is not something to be cured, but an integral part of their identity. The medical model is often critiqued by the social model of disability. The image below illustrates the two different models.

Information from "Disability Studies" in Sage Key Concepts: Key Concepts in Learning Disabilities .
Recommended Resources
- Michigan Disability Rights Coalition-Models of Disability The Michigan Disability Rights Coalition defines multiple theories of disability.
- << Previous: Home
- Next: Social/Independent Living Model >>
- Last Updated: Nov 9, 2023 9:11 AM
- URL: https://guides.library.illinois.edu/disabilitytheory

3 Models Underlying Assumptions About Disability
Backlash from disabled people about "the witches" reveals harmful stereotypes..
Posted November 12, 2020 | Reviewed by Matt Huston
Think about your underlying assumptions about disability. What causes disability? What are the sources of and solutions to disability-related challenges? Experts categorize ways of thinking about disability into three general models: moral , medical , or social (Olkin & Pledger, 2003). Our beliefs about disability are reflected in and perpetuated by media depictions .

Moral Model
This model encompasses beliefs that disabled people or their families are morally responsible for their disability. According to the moral model, disability is a punishment for sins, a representation of internal evils, a curse, or a result of karma. It is the reason why people with disabilities are still hidden away and kept a family secret in some cultures.
We might call the moral model archaic, but we still see evidence of this model in our culture today. Most recently, the movie The Witches has come under fire from the disability community for depicting the witches as having limb differences—three fingers on each hand and a single toe on each foot. The witches’ CG-created hands and feet mimic limb disabilities such as ectrodactyly. In his original book, Roald Dahl described the witches as having “cat-like" claws, and in the 1990 movie adaptation, the witches had long, pointed nails on five-fingered hands. So why the new look? In a statement , Warner Bros. said that they invited designers to reimagine the look of the witches for the new movie. Both Warner Bros. and Anne Hathaway , who plays the Grand High Witch, have released statements saying they did not make the connection between the witches’ appearance and disability. It may be true that the movie makers did not consciously see the resemblance; however, a modicum of research and input from the disability community would have revealed this is a recapitulation of a lazy and harmful trope. People with limb differences like Dr. David Garcia have responded with the hashtag #notawitch.
Hollywood has a long history of using physical differences as a symbol of villainy. Think of Dr. Poison in "Wonder Woman," Freddy Kruger, the Joker, and almost all Bond villains. The villains Scar from The Lion King and Captain Hook from Peter Pan are named after their visible differences. These depictions perpetuate cultural associations between visible difference and evil. Disabled activists have long advocated for more and more realistic representation in media.
Medical Model
The most common way of thinking about disability in Western cultures is the medical model. This view sees disability as the direct result of abnormalities in the body or mind, which it aims to cure. The medical model offers valuable innovations for treating painful symptoms. However, this model locates the problem within the disabled individual, and the responsibility for treating the disability is limited to the disabled person, their family, and an esoteric group of healthcare specialists. Limiting the responsibility of supporting disabled people to a small group perpetuates the idea that disability is an exception, rather than a common human experience. While the medical model is a step forward, our understanding of disability is incomplete until we consider social factors.
Social Model
Disability activists and scholars emphasize the role of society in constructing and defining normality. The social model asserts that society is the primary cause of disability, and the “problem” lies in society, not in the individual. Society’s lack of accommodation of human variation is viewed as the cause of the disabling experience (Olkin & Pledger, 2003). Disability occurs because societies are constructed based on the assumption that everyone functions according to a culturally defined norm.
For example, there is an impairment that more than half of Americans have, but we don’t consider it a disability. It’s refractive error (nearsightedness, farsightedness, etc.; Vitale et al., 2008). When I ask my students why using corrective lenses is not considered a disability, they usually say it’s because glasses and contacts are easy to make. But it’s not that it is inherently easy to create lenses, it’s that we were motivated to devote the resources to doing so. In fact, glasses may be the first assistive technology, developed in the 13th century (Ilardi, 2007). Lenses seem like simple accommodations because they are common, effective, and inexpensive. Our society values equality; we can and should do this for more human variations, regardless of how common or rare.
Disabled people are more likely to have a social model perspective than nondisabled people (Bogart et al., 2019). A classic social psychological concept may help explain why. The actor-observer effect indicates that we can recognize how the power of the situation shapes our own behavior, but when we observe the same behavior in others, we neglect to see the role of the environment and assume that a person is behaving that way because it is who they are (Dunn, 2019). For example, you are likely to blame someone else for being late to a meeting, making attributions about them as a person (e.g., they are irresponsible or don't respect your time). On the other hand, if you are late to a meeting, you are more likely to recognize the situational factors at play (e.g., your child woke up sick that morning, or a car accident stopped traffic). Similarly, this occurs for people with disabilities. Disabled people can readily recognize the social and environmental barriers (e.g., a major factor preventing employment of people with physical disabilities is a lack of accessible workplaces). People without disabilities, as observers, may assume that the problem is inherent in the person (e.g., viewing disabled people as lazy or incompetent).
Toward Inclusion
Our underlying assumptions about disability predict our attitudes and behaviors toward people with disabilities (Bogart et al., 2019). Moral model ideas perpetuate fear or disgust toward people with disabilities and can underlie decisions to keep disabled people hidden or separated from the rest of society (e.g., sheltered workshops, segregated special education classrooms). When exclusively adhered to, the medical model promotes the idea that the only “solution” to disability is a cure. This can lead disabled and nondisabled people alike to view anything less than a cure as a failure. The social model puts the onus of change on society to create an accessible and inclusive world.

People with disabilities may be the largest minority group in the United States, at 26% of the population , yet they are the most underrepresented in TV, movies, and the media at large. For example, only 3% of TV characters had a disability in the 2019-2020 season . When there are characters with disabilities, they are usually written and portrayed by non-disabled people, which can lead to inaccurate, stereotyped portrayals. However, there are some promising exceptions. For example, Ryan O'Connell, who has cerebral palsy, writes, produces, and stars in the hilariously dark Netflix series Special. Representing people with disabilities in the media as complex human beings is crucial to forming an inclusive society.
Bogart, K. R., Logan, S. W., Hospodar, C., & Woekel, E. (2019). Disability models and attitudes among college students with and without disabilities. Stigma and Health, 4(3), 260–263.
Dunn, D. S. (2019). Outsider privileges can lead to insider disadvantages: Some psychosocial aspects of ableism. Journal of Social Issues, 75(3), 665-682.
Ilardi, V. (2007). Renaissance Vision from Spectacles to Telescopes. United States: American Philosophical Society.
Olkin, R., & Pledger, C. (2003). Can disability studies and psychology join hands? American Psychologist, 58(4), 296.
Vitale, S., Ellwein, L., Cotch, M. F., Ferris, F. L., & Sperduto, R. (2008). Prevalence of refractive error in the United States, 1999-2004. Archives of ophthalmology, 126(8), 1111-1119.

Kathleen Bogart, Ph.D. , is an Associate Professor of Psychology at Oregon State University. She researches the implications of living with disability, rare disorders, or facial differences.
- Find a Therapist
- Find a Treatment Center
- Find a Psychiatrist
- Find a Support Group
- Find Online Therapy
- United States
- Brooklyn, NY
- Chicago, IL
- Houston, TX
- Los Angeles, CA
- New York, NY
- Portland, OR
- San Diego, CA
- San Francisco, CA
- Seattle, WA
- Washington, DC
- Asperger's
- Bipolar Disorder
- Chronic Pain
- Eating Disorders
- Passive Aggression
- Personality
- Goal Setting
- Positive Psychology
- Stopping Smoking
- Low Sexual Desire
- Relationships
- Child Development
- Self Tests NEW
- Therapy Center
- Diagnosis Dictionary
- Types of Therapy

At any moment, someone’s aggravating behavior or our own bad luck can set us off on an emotional spiral that threatens to derail our entire day. Here’s how we can face our triggers with less reactivity so that we can get on with our lives.
- Emotional Intelligence
- Gaslighting
- Affective Forecasting
- Neuroscience

Enabling America: Assessing the Role of Rehabilitation Science and Engineering (1997)
Chapter: 3 models of disability and rehabilitation, 3 models of disability and rehabilitation.
Models assist understanding by allowing one to examine and think about something that is not the real thing, but that may be similar to the real thing. People use a variety of models to obtain a clearer understanding of a problem or the world around them. Such models include physical models, three-dimensional graphical models, animal models of biological systems, mathematical or ideal models, and computer models. When relationships are highly complex, however, as they are in rehabilitation processes and other areas of human endeavor, it is seldom possible to develop models that are quantitatively predictive. Nevertheless, it is often possible to establish rough relationships between various variables that are observable.
Models based on partial knowledge are often called conceptual models. Conceptual models may help people to think about behaviors of components in complex systems, even though they may not yield quantitative answers. They may allow one to understand general relationships without the necessity for an extensive verbal or written description. In this way they are like an out-of-focus picture that partially reveals relationships. It is common in science and engineering to use models to help develop hypotheses that can be examined experimentally, but even as models assist scientists in moving forward with new understanding, they are abandoned for new versions. Experimental results may suggest that the models must be altered or even abandoned in favor of new models.
The models discussed in this chapter are conceptual in nature.
Such models must constantly be changed as new knowledge is gained if they are to adequately represent processes or systems that are in flux. Rehabilitation science and engineering, at its current stage of development, does not have a comprehensive paradigm or a universally accepted theoretical model. It is an emerging field of study, and as such, is still evolving. This chapter presents a brief look at the history of models of disability, which is useful in understanding the current status and direction of disability and rehabilitation research, and then presents a model of disability that builds upon and elaborates previous models, as well as adding several new elements. It presents this model verbally, schematically, and mathematically. Finally, it introduces a matrix that defines rehabilitation research.
Evolution of models of Disability
The prevailing wisdom about the causes of disability has changed in the last several decades. In the 1950s, impairment of a given severity was viewed as sufficient to result in disability in all circumstances; in contrast, the absence of impairment of that severity was thought to be sufficient grounds to deny disability benefits. Thus, the American Medical Association's Committee on Medical Rating of Physical Impairments stated that "competent evaluation of permanent impairment requires adequate and complete medical examination, accurate objective measure of function, and avoidance of subjective impressions and nonmedical factors such as the patient's age, sex and occupation" (American Medical Association, Committee on Medical Rating of Physical Impairment, 1958).
By the mid-1970s, Nagi (1976) outlined a process by which a pathology (e.g., arthritis) gave rise to an impairment (e.g., a limited range of motion in a joint), which may then result in a limitation in function (e.g., an inability to type), which, finally, may result in a disability (inability to work as a secretary). While outlining a process that would seem to move inexorably from pathology to loss of a job, Nagi noted that correlations among impairments, functional limitations, and work loss were poor, and he speculated that the extent to which the environment accommodated limitations largely determined whether disability would result from the onset of a medical condition. In the interim, at least three others have developed models or modifications: the WHO (International Classification of Impairments, Disabilities, and Handicaps, 1980), the IOM ( Disability in America, 1991), and the NCMRR (1993). All of these models attempt to facilitate and improve understanding by describing the concepts and relationships
among medical conditions, impairments, functional limitations, and the effects of the interaction of the person with the environment (i.e., handicap, disability, societal limitation) although each uses different nomenclatures for the components.
Nagi's model of disability explicitly brought the environment into the conceptualization. His model initiated a search for the factors in family, community, and society that affect disability as an outcome. With respect to disability in the work setting, for example, research has focused on the social and demographic characteristics of the individual and family, the individual's prior occupation and the industry in which the individual was previously employed, the flexibility of the workplace with respect to the physical tasks of work and hours of work, the nature of the local economy, customs and laws governing employment, and the extent of income transfer programs (Yelin, 1992).
Although the Nagi model included the environment, it was limited in how it conceived of the environment. In his model, the environment impinges on individuals only when activity limitation interacts with the demands placed on those individuals; the process that gives rise to disability is still inherently a function of the characteristics of medical conditions and attendant impairments.
The IOM model (IOM, 1991) was derived directly from Nagi, defining disability as "a function of the interaction of the person with the environment" and beginning to describe certain subsets of environmental factors that could potentially affect the development of and movement within a disabling process. In this model, physical and social environmental risk factors (as well as biological and lifestyle risk factors) were described as independent variables that exist at all stages of the process. These factors affect progression within the model, and their control therefore affects (prevents) disability.
The NCMRR model adds emphasis to the importance of environment by adding a category called societal limitations to account for restrictions that society places on individuals and that limit their ability to participate independently in tasks, activities, and roles. The unwillingness of employers to provide accommodations and the lack of ramps that deny access to public buildings to persons with disabilities are given as examples.
Building on these models, this committee describes a model where the environment interacts with the individual to determine whether disability will result. Nagi's nomenclature is used in describing the stages of the model and the relational nature of disability, as described in the IOM model, is now enhanced and clarified. In this new model, the environment plays a critical role in determining whether each stage occurs and if transitions between the stages occur.
A New Model for the Enabling-Disabling Process
A common understanding of such terms as injury, impairment, handicap, functional limitation, disabling conditions, and disability is essential to building effective, coherent programs in rehabilitation science and engineering. As described above, several frameworks have been advanced to describe disability-related concepts, but none of these has been universally adopted. The lack of a uniformly accepted conceptual foundation is an obstacle to research and to other elements critical to rehabilitation science and engineering. Using the definitions laid out in Chapter 1 , this committee presents a new set of models, based primarily on the previous IOM model (1991), designed to enhance the robustness of the previous models with respect to reversing the disabling process, i.e., rehabilitation. This section presents an overview of "the enabling-disabling process," explains its stages, and describes the nature of disability.
An Overview of the Enabling-disabling Process
An overview of how disabling conditions affect a person's access to the environment is shown in Figure 3-1 . Access to the environment, depicted as a square, represents both physical space and social structures (family, community, society). The person's degree of physical access to and social integration into the generalized environment is shown as degree of overlap of the symbolic person and the environmental square. A person who does not manifest disability (a) is fully integrated into society and therefore has full access to both: 1) social opportunities (employment, education, parenthood, leadership roles, etc.) and 2) physical space (i.e. space access equivalent to persons without disabling conditions). A person with potentially disabling conditions 1 has increased needs (expressed by the size of the individual) and is dislocated from their prior integration into the environment (b).
The rehabilitative process attempts to rectify this displacement, either by restoring function in the individual (c) or by expanding access to the environment (d) (e.g., building ramps). This model does not mean to imply that the two methods (which may be generally characterized as cure and care) are mutually exclusive. Indeed, the most effective rehabilitation programs include both. The model separates the two only to illustrate that disability is the interaction between the potentially disabling

FIGURE 3-1 Conceptual overview of the enabling-disabling process. The environment, depicted as a square, represents both physical space and social structures (family, community, society). A person who does not manifest a disability (a) is fully integrated into society and "fits within the square." A person with potentially disabling conditions has increased needs (expressed by the size of the individual) and is dislocated from his or her prior integration into the environment (b) that is, "doesn't fit in the square." The enabling (or rehabilitative) process attempts to rectify this displacement, either by restoring function in the individual (c) or by expanding access to the environment (d) (e.g., building ramps).
conditions of an individual and the environment, and therefore strategies that affect the environment or the pertinent potentially disabling conditions both target disability. While this model provides an overview, more detail is provided below.
The New IOM Model
Looking at the enabling-disabling process with more scrutiny requires greater detail in the model. To this end, this report adopts the IOM model (1991) and makes some modifications designed to both improve the model and to tailor it more towards rehabilitation (see Figure 3-2 ). The original IOM model was conceived with prevention in mind, and the need for identifying risk factors whose control would facilitate the prevention of disability. The 1991 IOM model (IOM, 1991) established a new conceptual foundation in the field of disability in that it analyzed and described the components of the disabling process in such a way as to allow for the identification of potential points for preventive intervention. Identifying and describing the importance of the different types of risk factors that affect the disabling process as well as the interaction and integral nature of quality of life were fundamental contributions to the emerging field of disability prevention. Over time, however, some shortcomings in the 1991 IOM model have emerged, including the implication that the disabling process is unidirectional, progressing inexorably toward disability without the possibility of reversal. The unidirectionality was implied by the arrows in the model that pointed only to the right, that is, toward the condition of disability. Although this may have been a result of that committee's focus on developing interventions to prevent progression in the disabling process rather than reversal, that is, rehabilitation, it is a shortcoming in the original model that needs correction and clarification, especially in the context of rehabilitation.
A second apparent shortcoming in the 1991 IOM model is its limited characterization of the environment and the interaction of the individual with the environment. Although the importance of the environment is discussed in the text in some detail, it is not clearly represented in the model except as a category of risk factors involved in the transition between the various categories of the disabling process.
The third apparent shortcoming in the 1991 IOM model that the committee identified as needing improvement is the representation of societal limitation. Some enhancements to the original model address these shortcomings.
The new IOM model (Figures 3-2 , 3-3 , and 3-4 ) is designed to show disability more clearly as the interaction of the person with the environ-

FIGURE 3-2 Modified IOM model. The Disability in America model (Institute of Medicine, 1991) is revised to include bidirectional arrows and a state of "no disabling condition," and to show transitional factors and quality of life interacting as part of the enabling-disabling process. The state of "disability" does not appear in this model since it is not inherent in the individual but, rather, a function of the interaction of the individual and the environment.

FIGURE 3-3 The person-environment interaction. The enabling-disabling process is depicted as being an active part of the individual person. The physical and social environments are depicted as a three-dimensional mat, with social factors on one side and physical factors on the other. The interaction of the person and the "environmental mat" is depicted as a deflection in the mat.
ment and also to show the possibility of movement in the direction of rehabilitation. To accomplish this diagrammatically, the new model is three-dimensional and has the following new features:
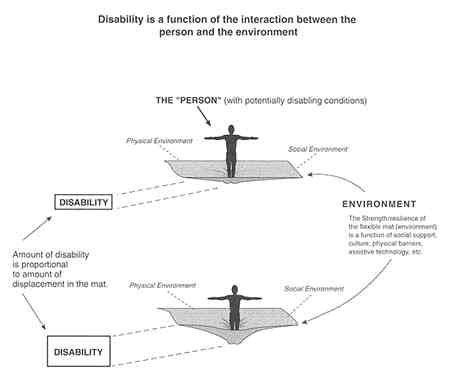
FIGURE 3-4 Disability as displacement of the environmental mat. The amount of disability that a person experiences is a function of the interaction between the person and the environment. The amount of displacement in the environmental mat is a function of the strength of the physical and social environments that support an individual and the magnitude of the potentially disabling condition. The amount of displacement represents the amount of disability that is experienced by the individual.
- has been moved from being a part of the disabling process to being a product of the interaction of the person with the environment.
Each of these enhancements is described in greater detail below.
Assembling the Model
As shown in Figure 3-3 , the new model can be shown as having three parts: the person, the environment, and the interaction of the person with the environment (disability).
The Person In the new model a new designation was added to indi-
cate people with no disabling conditions. This feature of the model will allow for ''complete" rehabilitation (designating also both the origin of the disabling process and the termination of the enabling process).
Transitional Factors In the new model, the committee defines the converse of risk factor as "enabling factor." Risk factors are phenomena that are associated with an increase in the likelihood that an individual will move from left to right in the new model, that is, from no disabling condition toward functional limitation. In contrast, enabling factors are phenomena that are associated with an increase in the likelihood that an individual will move from right to left in the new model, that is, toward less limitation.
The general types of enabling factors are the same as the general types of risk factors, that is, environmental (social, psychological, and physical) along with lifestyle and behavioral. So, for example, access to appropriate care and assistive technology would be an enabling factor (social environment), but lack of access would be a risk factor, or a disabling factor; curb cuts and universal design would be enabling factors (physical environment), but a lack of these would be disabling factors; the age of the person is a biological factor that can be either enabling or disabling; and compliance with pharmaceutical prescription regimens would be enabling, whereas drug abuse would be a disabling (behavioral and lifestyle) factor.
Thus, since both disabling and enabling factors affect transitions between the stages of the model, the committee groups them together as "transitional factors."
The Environment The environment is represented as a flexible three-dimensional mat in the new model. The strength and resilience of this mat are proportional to the quantity and quality of accessible support systems and the existence of various barriers. Stronger mats equate with more supportive environments, for example, access to appropriate health care, the availability of assistive technology and social support networks, and receptive cultures. Weaker mats equate with nonsupportive environments. For example, physical barriers, discrimination, lack of accessible and affordable assistive technology, and lack of appropriate health care result in greater displacement of the mat and, therefore, cause greater disability.
Thus, a person with a given level of impairment or functional limitation (i.e., potential disability) will experience greater disability (more displacement of the mat) in a less supportive environment than he or she would experience in a more supportive environment (indicated by a stronger mat and less resulting displacement). The amount of disability is pro-
portional to the amount of displacement in the mat that represents the environment.
The environment is represented as having two general categories: the social-psychological and the physical. Examples of the types of things that might be included in each category include:
Psychological and Social Environments
- Discrimination
- Access to health and medical care
- Appropriate care
- Access to technology
- Community organizations
- Access to social services
- Traits and personality factors
- Attitudes and emotional states
- Access to fitness and health-promoting activities
- Spirituality
- Independence
Physical Environments
- Architecture
- Transportation
- Appropriate technology
Each of the items listed in the social and physical environments could be thought of as layers in the mat; for example, access to assistive technology would be a layer in the environment mat, and so if an individual had good access to assistive technology, a strong layer for assistive technology would be added to the mat. If there were no access to assistive technology, then this layer would be missing from the mat, thus weakening the overall support and increasing the resultant disability.
In keeping with this model, it is important to note that the environment interacts at all points in the process (e.g., the environmental risk factors described in Disability in America [Institute of Medicine, 1991]).
Reflecting the increasing focus on the interaction of the individual
and the environment, recent research on disability and rehabilitation has described the constituent parts of the environment in as much detail as Nagi's model gave to the individual pathway (Fawcett et al., 1994; Fougeyrollas and Gray, 1996; Fougeyrollas, 1997; Law et al., 1996). These researchers see the environment of the person with a disabling condition as including elements that are proximate, such as the immediate home and work environments (termed the microsystem of the individual), and distal, such as the community in which the individual lives (termed the mesosystem ) and the society, economy, and, perhaps above all, the culture in which the local community is embedded (termed the macrosyste ) . However, these researchers do not include psychological or intrapersonal factors as part of the microsystem, an omission that the enhancements of the model described in this chapter are meant to rectify. In this chapter, psychological factors such as one's thoughts, beliefs, or expectancies are included in the intrapersonal environment.
Although the person with a disabling condition experiences the microsystem tangibly every day, the extent to which a particular condition is expressed as a disabling condition may be determined as much at the macro- or mesosystem level as by the nature of the local environment. For example, research on disability in the work setting indicates that the economic status of the overall labor market has a far greater impact on the employment status of people with disabling conditions than the willingness of individual employers to provide accommodations or the extent of the physical or mental impairment for that matter, even though both accommodations and extent of impairment do have some effect (Yelin, 1992). Similarly, the overall culture frequently determines whether a limitation will be considered disabling. In the broader U.S. culture, for example, a severe limitation in hearing is considered a disability. In a society in which the culture supports the use of sign language, a hearing loss may not be limiting (Groce, 1985).
The relative importance of the different elements of the environment may differ among kinds of activities. The extent of family help and the nature of the landscape and the built environment—microsystem and mesosystem characteristics, respectively—may affect an individual's ability to get around the community more than the overall culture (macrosystem characteristics). Even in that example, however, the importance of the overall culture becomes clear, because in some societies the provision of such services flows quite naturally from a communitarian ethos, whereas in others it is left to individuals and families to fend for themselves.
Disability The definition of disability has not changed, but its representation in the model has. In the new model, disability is a dependent variable whose value is determined by the relationship between two other
variables: the person and the environment. Since disability is not a part of the person, but rather is a function of the interaction of the person with the environment, the box that represented disability in the 1991 IOM model has been removed from the person component in the new model (see Figure 3-4 ). Disability is now represented as the quantity of deflection in the mat that represents the environment.
Thus, in the new model disability is a relational outcome. Although many parts of the process are not well understood at present, the areas in which knowledge is strong and those in which it is weak can be specified in the new model.
Theoretical Quantification and Mathematical Model of Disability
As a relational concept, disability lends itself to mathematical modeling. At present this can be done only on a conceptual basis, since quantification of the variables is not yet reliable and reproducible. Nonetheless, a mathematical model is useful in further clarifying the relationship that exists between the person and the environment and how they interact to create disability.
Beginning with the variables of pathology (P), impairment (I), and functional limitation (FL), the first assumption is that the sum of these variables represents a quantity known as an individual's potential disability, or PD: P + I + FL = PD. Potential disability is referred to as "potential" because it is only the interaction of potential disability with the environment that creates true disability. In addition, some (or all) of these variables may be equal to zero. If all are equal to zero, then there is no potential disability.
Environment (E) is the denominator in the mathematical model, because it is the influence of the environment that creates disability from any given potential. The environment is the variable factor against which the other factors are measured and that determines the existence of disability. Without environmental factors there would be no disability. Thus, disability (D) can be represented mathematically as the relationship of potential disability (PD, or P + I + FL) to environment (E): (P + I + FL)/E = D or PD/E = D.
Take the following example. If the range of PD (i.e., the sum of P + I + FL ) is 0 to 10 (where 10 is the maximum potential for experiencing disability) and the range of E is 0.1 to 10 (where 1.0 is a neutral environment, 10 is a very accessible and supportive environment, and 0.1 is a very inaccessible and nonsupportive environment), then the resultant quantity of D would range from 0 to 100 (where 100 is maximum disability).
So, for example, if PD were 5 and the environment were a very "good"
TABLE 3-1 Estimating the Effects of the Environment on Disability
one (e.g., E = 10), then the level of disability would be 0.5. However, with the same PD (i.e., PD = 5) but a less supportive environment (e.g., E = 1), then the level of disability would increase from 0.5 to 5. (When E is equal to 1, the effect of the environment is neutral and PD is equal to D. )
Mathematically, to allow the environment to exert a truly negative effect in the model, the range of quantities for the denominator (i.e., the environment) should be less than 1.0 but greater than zero; thus, the range would be from 0.1 to 10. Using the example above, if E is equal to 0.5 instead of 1, then the level of disability would increase from 5 to 10. If the environment was at its worst (i.e., E = 0.1), then the amount of disability would increase to 50 in this example.
In summary, maintaining the level of potential disability constant ( PD = 5) and varying the quality of the environment ( E is from 0.1 to 10) results in the moderate disability scores listed in Table 3-1 for the example cited above.
Conceptual Matrix for Rehabilitation Research
The conceptual models presented here could form the basis for a new science—rehabilitation science and engineering—that embodies the underlying, rudimentary paradigm implicit in each. The committee believes that there is a legitimate and distinct field of study that justifies the term "rehabilitation science." Rehabilitation science emphasizes function, focusing on the processes by which disability develops and the factors in-
fluencing these processes. The vision of rehabilitation science is that better understanding of the causes and factors contributing to disability will lead to better treatments and technology for those with disabling conditions. To help define the parameters of rehabilitation science and engineering, the committee developed the conceptual matrix presented in Table 3-2 . The matrix is useful as a tool for identifying the focus of rehabilitation science and engineering, defining which research activities address rehabilitation, and providing new possibilities for future research.
Table 3-2 demonstrates that rehabilitation science and engineering targets the enabling-disabling process, which runs across the stages of disability, and addresses the disabling conditions and the environment. The cells of this matrix (i.e., the different letters, A l through M 4 ) match disability-related variables in the rows to performance measures in the columns. A single cell (e.g., A l or C 3 ) in the matrix constitutes the minimum requirement for research classified as associated with the new academic field of rehabilitation science and engineering. If a row variable is studied across several performance states, the multi-cell begins to represent the enabling-disabling process. Every research study in rehabilitation science and engineering must have some measure of disability-related function (columns) and some measure of a disability-related variable, either of the person or of the environment (rows). It is not sufficient to study a classification of illness or disease without a measure of performance. This requirement defines the subset of pathology and pathophysiology research in medicine that overlaps with rehabilitation science and engineering. It also serves as a guide for defining the rehabilitation science and engineering relevant research in basic biological, physical, behavioral, and social sciences and in the health professional and engineering disciplines. The highest priority in rehabilitation science and engineering is for studies yielding causal explanations of disabling and rehabilitative processes.
The matrix also reveals the unique nature of rehabilitation science and engineering. First, rehabilitation science emphasizes function. Second, rehabilitation science focuses on factors that lead to transitions between pathology, impairments, functional limitation, and disability. Third, rehabilitation science examines physical, behavioral, environmental, and societal factors that influence these transitions. Although rehabilitation science is multidisciplinary and utilizes methods from many fields including medicine, biomedical engineering, material sciences, sociology, architecture, and even economics, it is distinct from other scientific disciplines due to its emphasis on function, factors, and interventions that disable or enable people. Rehabilitation science and engineering combines knowledge from these otherwise distinct disciplines to create a knowledge structure for the understanding of performance deficits un-
TABLE 3-2 Conceptual Parameters of Rehabilitation Science and Engineering
derlying disability, the processes in which disabling conditions develop, progress, and reverse, and the factors that mediate the disabling and enabling processes.
Table 3-2 finally creates possibilities for new research. The matrix identifies combinations of variables which can be researched, but are not likely studied in the separate, existing basic science, health professional, and engineering disciplines. The variables in the rows (i.e., person and environmental variables) may be investigated as dependent or independent variables with the performance realms (columns) as the respective independent or dependent variable counterpart. Switching the independent variable from column to row will allow elucidation of the impact of disabling or rehabilitative processes on the person or society, on the one hand, or the impact of person or environmental variables (as positive or negative effectors) on enabling and disabling processes. The new knowledge of rehabilitation science and engineering will stimulate insights into rehabilitative processes and innovations into rehabilitation therapeutics.
The matrix in Table 3-2 can also be used to evaluate current data collection efforts with respect to the prevalence of and impact of disability. Currently, federal surveys routinely collect information on the extent of pathology, impairments, and on limitations in major classifications of activities. The National Health Interview Survey collects some information on behavioral factors and in the use of health care. In addition, some episodic surveys such as the Longitudinal Study on Aging and Health and Retirement Survey collect some information on accommodations provided by government, family, and employers. However, no ongoing surveys routinely collect information on the experiential and resource domains within personal factors and none collect information on such external environmental factors as the natural and engineered environment, access to rehabilitation specific therapies and health care, the availability of social supports, and the experience of the laws and regulations governing disability policy. In short, information on disability is almost exclusively within the personal domains and even so, tends to focus on definitions of disability that accord with much more primitive models of disability.
Summary and Conclusions
The prevailing wisdom about the causes of disability has shifted dramatically in the span of the last several decades. From the deterministic position of the American Medical Association Committee on Impairments of the 1950s, in which pathology was viewed as equivalent to disability, to the probabilistic one in more recent years of Nagi, IOM, and National Center for Medical and Rehabilitation Research (NCMRR) that, although
still focusing on the characteristics of the individual, viewed the relationship among pathology, impairment, functional limitation, and disability as contingent, to the view espoused here, that the environment and characteristics of the individual conjointly determine disability, the underlying notion of why someone is unable to function in the major activities of life has been transformed.
The notion that disability arises from the interaction of a person's physical condition and the person's environment has several implications. These implications affect research, professional training, and policy. Although there is not space here to discuss these implications in depth, their outlines will be sketched briefly in the hopes that others will investigate them further.
One implication of the notion that environments can be enabling is that disability does not always have to be viewed through a "deficit" model. Rather, it should be recognized that in an environment that is strongly enabling, a person with a substantial physical impairment can live a life that is indistinguishable in important ways from that of a similar person without such an impairment. That is, the person with the impairment can hold a good job, be married and have a family, engage in non-work-related activities, enjoy social relationships, and be part of a community. Not much research has been done from this perspective. Some exceptions are the works of Gray (1996), and White et al. (1995). The committee strongly recommends that more research be done which emphasizes the effects of enabling environments on the lives of people with impairments and functional limitations. If disability is a function of the environment, it is not a stable attribute across situations. Rather, it will depend on the particular environment or the particular situation. For example, it is possible that a person with a certain type of impairment might be more disabled in his or her work environment than in the family environment. This would be true, for example, of a deaf person working with hearing coworkers who did not know how to sign, who worked for a company that provided interpreters only for large or important meetings, but whose spouse and children all signed fluently. Or an impairment might affect a person's ability to use public transportation, but not the ability to work once arriving in the workplace.
For research, this means that one measurement of impairment or functional limitation cannot be developed to indicate degree of disability in all situations. One measurement that attempts to indicate how disabled a person is would be misleading. If the measurement were limited to a specific, clearly defined situation, such as a workplace, it might be possible to include enough environmental indicators that a valid and reliable measurement might be developed; however, this measurement
is unlikely to apply across all situations. This will, for the short run, make the tasks facing researchers much harder.
This conception of disability also carries with it implications for professional training. If the goal of professional training in rehabilitation is to impart the skills needed to reduce disability, training programs will need to teach many forms of environmental modification. Training may need to be broader than it has been, and it will need to include more professional fields and skills (see Chapter 9 for further discussion of this issue).
Finally, even though disability policy is not the focus of this report, it is worth noting that the policy implications arising from this definition of the concept are enormous. Disability determination will not be able to be a single event. Rather, a determination of disability status, for example, for the purpose of receiving Social Security Disability Income benefits, will have to be tied to a specific time, place, set of skills, and type of job. It cannot be permanent, for not only will changes in the person's own health or educational status change it, but so will changes in aspects of the work environment. Additionally, any single disability determination might not be acceptable across programs, since different programs apply to different environments.
Recommendations
Recommendation 3.1 Researchers and educators should adopt the model for rehabilitation and the enabling-disabling process presented here. Programs supporting rehabilitation-related research should adopt its terminology and use it as an organizing tool.
Recommendation 3.2 Based on the model of the enabling-disabling process described in this report, methods for quantifying disability should be developed that are sensitive to the characteristics of both the person and the environment. Such a metric would facilitate additional research into the factors that affect transitions between disability and other states of the enabling-disabling process, and the development of effective preventive and rehabilitative intervention strategies.
The most recent high-profile advocate for Americans with disabilities, actor Christopher Reeve, has highlighted for the public the economic and social costs of disability and the importance of rehabilitation. Enabling America is a major analysis of the field of rehabilitation science and engineering. The book explains how to achieve recognition for this evolving field of study, how to set priorities, and how to improve the organization and administration of the numerous federal research programs in this area.
The committee introduces the "enabling-disability process" model, which enhances the concepts of disability and rehabilitation, and reviews what is known and what research priorities are emerging in the areas of:
- Pathology and impairment, including differences between children and adults.
- Functional limitations—in a person's ability to eat or walk, for example.
- Disability as the interaction between a person's pathologies, impairments, and functional limitations and the surrounding physical and social environments.
This landmark volume will be of special interest to anyone involved in rehabilitation science and engineering: federal policymakers, rehabilitation practitioners and administrators, researchers, and advocates for persons with disabilities.
READ FREE ONLINE
Welcome to OpenBook!
You're looking at OpenBook, NAP.edu's online reading room since 1999. Based on feedback from you, our users, we've made some improvements that make it easier than ever to read thousands of publications on our website.
Do you want to take a quick tour of the OpenBook's features?
Show this book's table of contents , where you can jump to any chapter by name.
...or use these buttons to go back to the previous chapter or skip to the next one.
Jump up to the previous page or down to the next one. Also, you can type in a page number and press Enter to go directly to that page in the book.
Switch between the Original Pages , where you can read the report as it appeared in print, and Text Pages for the web version, where you can highlight and search the text.
To search the entire text of this book, type in your search term here and press Enter .
Share a link to this book page on your preferred social network or via email.
View our suggested citation for this chapter.
Ready to take your reading offline? Click here to buy this book in print or download it as a free PDF, if available.
Get Email Updates
Do you enjoy reading reports from the Academies online for free ? Sign up for email notifications and we'll let you know about new publications in your areas of interest when they're released.
Importance of the Social Model of Disability Essay
- To find inspiration for your paper and overcome writer’s block
- As a source of information (ensure proper referencing)
- As a template for you assignment
People’s perceptions concerning individuals with disabilities determine how they care and live with them in different communities. In this regard, the social model of disability focuses on changing the misconception that people with disabilities have problems, which need medical treatments to be fixed. According to Kattari et al. (2017), the model highlights society’s barriers and blame them for the anguishes experienced by persons with disabilities. Indeed, although they strive to live a prosperous life, external forces rather than medical reasons interrupt their progress and ambitions. For example, it is significant to examine environmental challenges, including buildings, public places, and modes of transport developed without thoughts of people with disabilities’ needs. Therefore, the social model helps individuals visualize the building’s problem for lacking a ramp at the entrance instead of blaming people for their disabilities, which are beyond their control.
Besides, the social model helps eliminate prejudices and stereotypes that prevent disabled individuals from enjoying equal opportunities as other humans in society. For instance, the public perceives people with disabilities as dependents and burdens to their families and communities. Such misunderstandings have inspired negative attitudes, including assuming that a person with a disability cannot work, live independently, and have children (Kattari et al., 2017). The social model helps to change the public conversation and create an environment that guarantees the choice, control, and independence of disabled individuals. In this way, the government and its people can focus on solutions, which eliminate discriminatory conclusions restricting the potential of persons with disabilities. Additionally, the social model encourages the formulation of flexible policies, which incorporate empathy and safeguard all individuals’ rights in society, irrespective of their physical or emotional incapacities. Conclusively, the model suggests solutions that rectify the problems witnessed in the modern and disabling world to remove barriers, which discriminate and isolate people with disabilities.
Kattari, S. K., Lavery, A., & Hasche, L. (2017). Applying a social model of disability across the life span. Journal of Human Behavior in the Social Environment , 27 (8), 865-880. Web.
- Human Cloning Technology and Its Justification
- Child Abuse Versus Elder Abuse
- Safety Management System: Airport Ramps in the UAE
- Social Work as an Important Element of Society
- The Role of a Student in Society
- Changing Attitudes Toward Sickness and the Sick
- Examining Whitfield County
- Unruly Youth in Urban Environments. Analysis
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2022, February 23). Importance of the Social Model of Disability. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/
"Importance of the Social Model of Disability." IvyPanda , 23 Feb. 2022, ivypanda.com/essays/importance-of-the-social-model-of-disability/.
IvyPanda . (2022) 'Importance of the Social Model of Disability'. 23 February.
IvyPanda . 2022. "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
1. IvyPanda . "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
Bibliography
IvyPanda . "Importance of the Social Model of Disability." February 23, 2022. https://ivypanda.com/essays/importance-of-the-social-model-of-disability/.
Ashley Graham: The Words I Use to Encourage Self-Love

I was 9 years old when I was first confronted with the idea of beauty . I’d always been a larger kid—stout, athletic. People would tell me I was “big and strong.” But this girl, a stranger I saw one day at Target—she was different. She had long, thin legs, a flat tummy, and grown-up breasts. Her blonde hair fell perfectly down her shoulders. I was so young, and yet I knew: she was pretty . I wanted to be that. I didn’t know what modeling was back then—I didn’t even know what fashion was—but I wanted what she had. I wanted to command attention.
My story began like so many women’s, as my sense of self evolved under the influence of feedback from others . In middle school the kids called me “cottage cheese thighs.” I craved acceptance of others and the empathy of a friend group that might understand what I had to offer beyond my exterior.
And then, suddenly, I was a model. A scout spotted me at the mall in Omaha when I was 12. Soon I was being paid to have my picture taken. Adults were telling me that my looks had value.
It came with a caveat, though. I was “big pretty” or “pretty for a big girl” or “pretty from the neck up.” There was always that double label: pretty and plus-sized . In school, the plus-size wasn’t cool, but the pretty was interesting. My teachers would tilt their heads and squint at me, looking for whatever the industry saw. I would fly to modeling jobs in New York City over the weekend with my mom, and be back in school facing the name-calling on Monday. I wish I’d had a mentor back then—someone to help me understand my value and my purpose as a model. But there was no one I could look to and emulate, no one who’d gone through the same challenges to hold my hand and tell me that none of the noise mattered, that I just needed to keep moving forward.
Read More: The 5 Words That Help Me Accept My Body
Developing my confidence in my own beauty came later—and it’s something I still struggle with sometimes. There isn’t one top model who doesn’t live with some sort of insecurity. You could talk to any of them, and I bet they would tell you all about it. We’re constantly being picked apart, constantly being told what’s right with how we look and what’s wrong, how we aren’t meeting the bar, what we need to change about ourselves. It’s enough to make anyone want to give up, and I almost did once, early on. I was 18 years old, living in Manhattan under tremendous pressure to build a new kind of career in a hyper-competitive city with skyrocketing rent. And it was complicated to be a plus-size model at a younger age, because there was even more scrutiny on the messaging—there was a negative connotation that came with youth and obesity and what it might mean to promote body diversity . I felt like I had to work twice as hard as everyone else because I was different. One day I finally called my mom crying, looking in the mirror and just feeling like I couldn’t do it anymore. She told me something I’ll never forget: your body is going to change someone’s life. You have to keep going.
That was the “aha” moment for me. My mom helped me understand my purpose. As I let her words sink in, I thought about how for years I’d let other people tell me who I was. I needed to define my worth for myself. And I could use words, like my mom had, to do it.
Affirmations are a trendy concept now, but back then I’d never heard of them. I literally searched “better words for self,” and I discovered that this was a tool that had helped other people. I could come up with my own personal phrases to use to speak directly to my insecurities. This is what I landed on: I am bold. I am brilliant. I am beautiful. Bold because I’d always been told I was too much—too big, too loud, too much personality—but I knew that my intensity and presence is what would set me apart. Brilliant because I was diagnosed with ADHD and dyslexia in the fourth grade and never had the resources I needed to really thrive in school—but I knew that I was smart and capable. Beautiful because I was starting to learn the fuller definition of the word, that beauty is about so much more than the parts of myself that were commoditized.
I used that affirmation for more than a decade as a tool to develop my self-love. Now I know I’m bold, brilliant, and beautiful, and I’ve moved on to other words. That doesn’t mean I don’t still suffer from waves of imposter syndrome or have hard days though. My body has changed things for other people, and there’s an incredible honor—and an incredible pressure—that comes with knowing that. I’ve always wanted women to see themselves in me, to know that any validation I get is equally theirs. But sharing my body with the world has also meant that the people I’ve set out to represent sometimes assume an ownership over my appearance. We all change . I was 28 when I appeared on the cover of Sports Illustrated Swimsuit . Now I’m 36 and a mother of three. My body looked different when I was pregnant, and it looks different now that I’ve given birth to my three sons. Losing weight after having kids has brought on comments from people who feel betrayed by the changes they see. I never want women to think I’m leaving them behind, and at the same time, all I can do is accept the journey I’m on and to focus on the things that make me feel strong and empowered—which is all any of us can do. Maybe I’ll lose weight, maybe I’ll gain it. This is my body, and I’m incredibly proud of everything it has accomplished.
That’s what beauty is. It’s knowing who you are, for better or worse, and loving yourself anyway. It’s learning and exploring and forgiving ourselves for the ways in which we differ. It’s grace.
Ashley Graham is a model, activist, author, and a member of the 2017 TIME100 . Her latest book is A Kids Book About Beauty .
—As told to Lucy Feldman
- How Joe Biden Leads
- TIME100 Most Influential Companies 2024
- Javier Milei’s Radical Plan to Transform Argentina
- How Private Donors Shape Birth-Control Choices
- What Sealed Trump’s Fate : Column
- Are Walking Pads Worth It?
- 15 LGBTQ+ Books to Read for Pride
- Want Weekly Recs on What to Watch, Read, and More? Sign Up for Worth Your Time
Contact us at [email protected] .

We Must Put an End to AI’s Culture of Secrecy
No, today’s ai isn’t sentient. here’s how we know, why i left billions on the table to fight for climate change, motherhood in a wheelchair isn't easy. but my disability will be my son's strength, how the world is failing victims of conflict-related sexual violence, we shouldn’t have to be willing to die to give birth in the u.s..
IMAGES
VIDEO
COMMENTS
8 The social model argued that disability was a status imposed on people with various forms of impairment, and therefore that disability was a political, not a health, issue. Social model proponents held that the medical model viewed personal impairment as the sole cause of disability, making an individual's body the appropriate target for ...
The medical model of disability often is depicted in movies through a plot in which a disabled person is depressed and hopeless, but through friendship with an able-bodied person the disabled person learns to embrace life. A reverse twist on this is the idea that disabled people show able-bodied characters how to be better people.
The development of the law in the United Kingdom is predominantly based on disability theories that challenge disability discrimination with reference to mechanisms that label disability as a problem in need of a solution, rather than recognition of disability as different but equal (Goodley et al., 2011).This is in contrast to the more radical models associated with feminism, queer theory and ...
Early scholarship distinguishes the medical model of disability, which locates physical and mental impairments in individual bodies, from the social model, which understands the world as disabling people. ... This essay considers how disability has been used as a justification for the oppression of marginalized populations. For example, slaves ...
The medical model of disability, or medical model, is based in a biomedical perception of disability. This model links a disability diagnosis to an individual's physical body. The model supposes that this disability may reduce the individual's quality of life and aims to diminish or correct this disability with medical intervention.
The medical model, as I formulate it, defines disability as an enduring biological dysfunction that causes its bearer a significant degree of impairment. I begin, in the next section, by outlining three desiderata for a theory of disability. Then, in Sect. 3, I explain the medical model's criteria for determining what counts as a disability ...
The social model's foil, and on some accounts its antithesis, is the medical model of disability. Both models treat disability as a locus of difficulties. While the medical model takes disability to be a problem requiring medical intervention—and as both the prerogative and the responsibility of medical professionals to fix—the social
The social model's foil, and on some accounts its antithesis, is the medical model of disability. Both models treat disability as a locus of difficulties. While the medical model takes disability to be a problem requiring medical intervention—and as both the prerogative and the responsibility of medical professionals to fix—the social ...
Origins of the term medical model. The term 'medical model of disability' was coined by a psychiatrist, Dr. Szasz, in the mid-1950s to critique the emerging psychiatric practice of defining mental conditions as illnesses and treating these new 'diseases' with medications (Hogan Citation 2019a).People with mental health conditions had long been considered deviant and abnormal (Lemert ...
by the medical model of disability. It is this medical model that has informed the development and structure of the legislation, and is reflected in people's attitudes and associated negative outcomes. Aspects of the Equality Act 2010 (the Act), in relation to disability discrimination, follow the medical model of disability as they focus on ...
The social model of disability says that disability is caused by the way society is organised. The medical model of disability says people are disabled by their impairments or differences. Under the medical model, these impairments or differences should be 'fixed' or changed by medical and other treatments, even when the impairment or ...
model of disability is the idea that disabilities are essentially. a test of faith or even salvific in nature. Niemann (2005:106) offers a concise description of the conception of disability as ...
The medical model of disability focuses on the medical aspects of a disability and seeks to "cure" a person of their disability so that they can return as closely as possible to a able-bodied state. In the past and even today, this is a common way that people think about disability. The problem is contained in the individual who has the ...
Further, we present practical examples using different hypothetical scenarios involving the same student with disabilities to depict how a teacher with a medical model orientation compared to a teacher with a social model orientation would interact and work with a student with a disability in physical education.
Medical Model. The most common way of thinking about disability in Western cultures is the medical model. This view sees disability as the direct result of abnormalities in the body or mind, which ...
The social model of disability the social model is a concept which recognises that some individuals have physical or psychological differences which can affect their ability to function in societies. (Brain.HE 2006) The medical model is used for those that need help. It is with the medical model that people can get support.
The medical model and the social model of disability are seen as mutually exclusive and jointly exhaustive; this is the view that disability is either caused by health impairments or by social circumstances, but not by both together nor by other factors. Received: November 15, 2017; Accepted: November 27, 2017; Published: November 30, 2017 Disability - physical or other, such as mental [1 ...
There are two main models of disability, the medical model and the social model. The medical model of disability, sees disabled people's inability to join in society as a direct result of having an impairment and not as the result of features of our society which can be changed (Swain, French, and Cameron, 2003).The World Health Organisation ...
among medical conditions, impairments, functional limitations, and the effects of the interaction of the person with the environment (i.e., handicap, disability, societal limitation) although each uses different nomenclatures for the components. ... Thus, in the new model disability is a relational outcome. Although many parts of the process ...
The human rights model focuses on the inherent dignity of the human being and subsequently, but only if necessary, on the person's medical characteristics. It places the individual centre stage in all decisions affecting him/her and, most importantly, locates the main 'problem' outside the person and in society. 9.
The social model helps to change the public conversation and create an environment that guarantees the choice, control, and independence of disabled individuals. In this way, the government and its people can focus on solutions, which eliminate discriminatory conclusions restricting the potential of persons with disabilities.
The model writes a personal essay on her evolving definition of beauty. ... But My Disability Will Be My Son's Strength. How the World Is Failing Victims of Conflict-Related Sexual Violence.