Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.

13.1 Sociological Perspectives on Health and Health Care
Learning objective.
- List the assumptions of the functionalist, conflict, and symbolic interactionist perspectives on health and medicine.
Before discussing these perspectives, we must first define three key concepts—health, medicine, and health care—that lie at the heart of their explanations and of this chapter’s discussion. Health refers to the extent of a person’s physical, mental, and social well-being. As this definition suggests, health is a multidimensional concept. Although the three dimensions of health just listed often affect each other, it is possible for someone to be in good physical health and poor mental health, or vice versa. Medicine refers to the social institution that seeks to prevent, diagnose, and treat illness and to promote health in its various dimensions. This social institution in the United States is vast, to put it mildly, and involves more than 11 million people (physicians, nurses, dentists, therapists, medical records technicians, and many other occupations). Finally, health care refers to the provision of medical services to prevent, diagnose, and treat health problems.
With these definitions in mind, we now turn to sociological explanations of health and health care. As usual, the major sociological perspectives that we have discussed throughout this book offer different types of explanations, but together they provide us with a more comprehensive understanding than any one approach can do by itself. Table 13.1 “Theory Snapshot” summarizes what they say.
Table 13.1 Theory Snapshot
| Theoretical perspective | Major assumptions |
|---|---|
| Functionalism | Good health and effective medical care are essential for the smooth functioning of society. Patients must perform the “sick role” in order to be perceived as legitimately ill and to be exempt from their normal obligations. The physician-patient relationship is hierarchical: The physician provides instructions, and the patient needs to follow them. |
| Conflict theory | Social inequality characterizes the quality of health and the quality of health care. People from disadvantaged social backgrounds are more likely to become ill and to receive inadequate health care. Partly to increase their incomes, physicians have tried to control the practice of medicine and to define social problems as medical problems. |
| Symbolic interactionism | Health and illness are : Physical and mental conditions have little or no objective reality but instead are considered healthy or ill conditions only if they are defined as such by a society. Physicians “manage the situation” to display their authority and medical knowledge. |
The Functionalist Approach
As conceived by Talcott Parsons (1951), the functionalist perspective emphasizes that good health and effective medical care are essential for a society’s ability to function. Ill health impairs our ability to perform our roles in society, and if too many people are unhealthy, society’s functioning and stability suffer. This was especially true for premature death, said Parsons, because it prevents individuals from fully carrying out all their social roles and thus represents a “poor return” to society for the various costs of pregnancy, birth, child care, and socialization of the individual who ends up dying early. Poor medical care is likewise dysfunctional for society, as people who are ill face greater difficulty in becoming healthy and people who are healthy are more likely to become ill.
For a person to be considered legitimately sick, said Parsons, several expectations must be met. He referred to these expectations as the sick role . First, sick people should not be perceived as having caused their own health problem. If we eat high-fat food, become obese, and have a heart attack, we evoke less sympathy than if we had practiced good nutrition and maintained a proper weight. If someone is driving drunk and smashes into a tree, there is much less sympathy than if the driver had been sober and skidded off the road in icy weather.
Second, sick people must want to get well. If they do not want to get well or, worse yet, are perceived as faking their illness or malingering after becoming healthier, they are no longer considered legitimately ill by the people who know them or, more generally, by society itself.
Third, sick people are expected to have their illness confirmed by a physician or other health-care professional and to follow the professional’s instructions in order to become well. If a sick person fails to do so, she or he again loses the right to perform the sick role.

Talcott Parsons wrote that for a person to be perceived as legitimately ill, several expectations, called the sick role, must be met. These expectations include the perception that the person did not cause her or his own health problem.
Nathalie Babineau-Griffith – grand-maman’s blanket – CC BY-NC-ND 2.0.
If all these expectations are met, said Parsons, sick people are treated as sick by their family, their friends, and other people they know, and they become exempt from their normal obligations to all these people. Sometimes they are even told to stay in bed when they want to remain active.
Physicians also have a role to perform, said Parsons. First and foremost, they have to diagnose the person’s illness, decide how to treat it, and help the person become well. To do so, they need the cooperation of the patient, who must answer the physician’s questions accurately and follow the physician’s instructions. Parsons thus viewed the physician-patient relationship as hierarchical: the physician gives the orders (or, more accurately, provides advice and instructions), and the patient follows them.
Parsons was certainly right in emphasizing the importance of individuals’ good health for society’s health, but his perspective has been criticized for several reasons. First, his idea of the sick role applies more to acute (short-term) illness than to chronic (long-term) illness. Although much of his discussion implies a person temporarily enters a sick role and leaves it soon after following adequate medical care, people with chronic illnesses can be locked into a sick role for a very long time or even permanently. Second, Parsons’s discussion ignores the fact, mentioned earlier, that our social backgrounds affect the likelihood of becoming ill and the quality of medical care we receive. Third, Parsons wrote approvingly of the hierarchy implicit in the physician-patient relationship. Many experts say today that patients need to reduce this hierarchy by asking more questions of their physicians and by taking a more active role in maintaining their health. To the extent that physicians do not always provide the best medical care, the hierarchy that Parsons favored is at least partly to blame.
The Conflict Approach
The conflict approach emphasizes inequality in the quality of health and of health-care delivery (Weitz, 2013). As noted earlier, the quality of health and health care differs greatly around the world and within the United States. Society’s inequities along social class, race and ethnicity, and gender lines are reproduced in our health and health care. People from disadvantaged social backgrounds are more likely to become ill, and once they do become ill, inadequate health care makes it more difficult for them to become well. As we will see, the evidence of disparities in health and health care is vast and dramatic.
The conflict approach also critiques efforts by physicians over the decades to control the practice of medicine and to define various social problems as medical ones. Physicians’ motivation for doing so has been both good and bad. On the good side, they have believed they are the most qualified professionals to diagnose problems and to treat people who have these problems. On the negative side, they have also recognized that their financial status will improve if they succeed in characterizing social problems as medical problems and in monopolizing the treatment of these problems. Once these problems become “medicalized,” their possible social roots and thus potential solutions are neglected.
Several examples illustrate conflict theory’s criticism. Alternative medicine is becoming increasingly popular, but so has criticism of it by the medical establishment. Physicians may honestly feel that medical alternatives are inadequate, ineffective, or even dangerous, but they also recognize that the use of these alternatives is financially harmful to their own practices. Eating disorders also illustrate conflict theory’s criticism. Many of the women and girls who have eating disorders receive help from a physician, a psychiatrist, a psychologist, or another health-care professional. Although this care is often very helpful, the definition of eating disorders as a medical problem nonetheless provides a good source of income for the professionals who treat it and obscures its cultural roots in society’s standard of beauty for women (Whitehead & Kurz, 2008).
Obstetrical care provides another example. In most of human history, midwives or their equivalent were the people who helped pregnant women deliver their babies. In the nineteenth century, physicians claimed they were better trained than midwives and won legislation giving them authority to deliver babies. They may have honestly felt that midwives were inadequately trained, but they also fully recognized that obstetrical care would be quite lucrative (Ehrenreich & English, 2005).

According to conflict theory, physicians have often sought to define various social problems as medical problems. An example is the development of the diagnosis of ADHD, or attention deficit/hyperactivity disorder.
birgerking – What I Really Do… ADD/ADHD – CC BY 2.0.
In a final example, many hyperactive children are now diagnosed with ADHD, or attention deficit/hyperactivity disorder. A generation or more ago, they would have been considered merely as overly active. After Ritalin, a drug that reduces hyperactivity, was developed, their behavior came to be considered a medical problem and the ADHD diagnosis was increasingly applied, and tens of thousands of children went to physicians’ offices and were given Ritalin or similar drugs. The definition of their behavior as a medical problem was very lucrative for physicians and for the company that developed Ritalin, and it also obscured the possible roots of their behavior in inadequate parenting, stultifying schools, or even gender socialization, as most hyperactive kids are boys (Conrad, 2008; Rao & Seaton, 2010).
Critics say the conflict approach’s assessment of health and medicine is overly harsh and its criticism of physicians’ motivation far too cynical. Scientific medicine has greatly improved the health of people around the world. Although physicians are certainly motivated, as many people are, by economic considerations, their efforts to extend their scope into previously nonmedical areas also stem from honest beliefs that people’s health and lives will improve if these efforts succeed. Certainly there is some truth in this criticism of the conflict approach, but the evidence of inequality in health and medicine and of the negative aspects of the medical establishment’s motivation for extending its reach remains compelling.
The Symbolic Interactionist Approach
The symbolic interactionist approach emphasizes that health and illness are social constructions . This means that various physical and mental conditions have little or no objective reality but instead are considered healthy or ill conditions only if they are defined as such by a society and its members (Buckser, 2009; Lorber & Moore, 2002). The ADHD example just discussed also illustrates symbolic interactionist theory’s concerns, as a behavior that was not previously considered an illness came to be defined as one after the development of Ritalin. In another example first discussed in Chapter 7 “Alcohol and Other Drugs” , in the late 1800s opium use was quite common in the United States, as opium derivatives were included in all sorts of over-the-counter products. Opium use was considered neither a major health nor legal problem. That changed by the end of the century, as prejudice against Chinese Americans led to the banning of the opium dens (similar to today’s bars) they frequented, and calls for the banning of opium led to federal legislation early in the twentieth century that banned most opium products except by prescription (Musto, 2002).
In a more current example, an attempt to redefine obesity is now under way in the United States. Obesity is a known health risk, but a “fat pride” or “fat acceptance” movement composed mainly of heavy individuals is arguing that obesity’s health risks are exaggerated and calling attention to society’s discrimination against overweight people. Although such discrimination is certainly unfortunate, critics say the movement is going too far in trying to minimize obesity’s risks (Diamond, 2011).
The symbolic interactionist approach has also provided important studies of the interaction between patients and health-care professionals. Consciously or not, physicians “manage the situation” to display their authority and medical knowledge. Patients usually have to wait a long time for the physician to show up, and the physician is often in a white lab coat; the physician is also often addressed as “Doctor,” while patients are often called by their first name. Physicians typically use complex medical terms to describe a patient’s illness instead of the more simple terms used by laypeople and the patients themselves.
Management of the situation is perhaps especially important during a gynecological exam, as first discussed in Chapter 12 “Work and the Economy” . When the physician is a man, this situation is fraught with potential embarrassment and uneasiness because a man is examining and touching a woman’s genital area. Under these circumstances, the physician must act in a purely professional manner. He must indicate no personal interest in the woman’s body and must instead treat the exam no differently from any other type of exam. To further “desex” the situation and reduce any potential uneasiness, a female nurse is often present during the exam.
Critics fault the symbolic interactionist approach for implying that no illnesses have objective reality. Many serious health conditions do exist and put people at risk for their health regardless of what they or their society thinks. Critics also say the approach neglects the effects of social inequality for health and illness. Despite these possible faults, the symbolic interactionist approach reminds us that health and illness do have a subjective as well as an objective reality.
Key Takeaways
- A sociological understanding emphasizes the influence of people’s social backgrounds on the quality of their health and health care. A society’s culture and social structure also affect health and health care.
- The functionalist approach emphasizes that good health and effective health care are essential for a society’s ability to function, and it views the physician-patient relationship as hierarchical.
- The conflict approach emphasizes inequality in the quality of health and in the quality of health care.
- The interactionist approach emphasizes that health and illness are social constructions; physical and mental conditions have little or no objective reality but instead are considered healthy or ill conditions only if they are defined as such by a society and its members.
For Your Review
- Which approach—functionalist, conflict, or symbolic interactionist—do you most favor regarding how you understand health and health care? Explain your answer.
- Think of the last time you visited a physician or another health-care professional. In what ways did this person come across as an authority figure possessing medical knowledge? In formulating your answer, think about the person’s clothing, body position and body language, and other aspects of nonverbal communication.
Buckser, A. (2009). Institutions, agency, and illness in the making of Tourette syndrome. Human Organization, 68 (3), 293–306.
Conrad, P. (2008). The medicalization of society: On the transformation of human conditions into treatable disorders . Baltimore, MD: Johns Hopkins University Press.
Diamond, A. (2011). Acceptance of fat as the norm is a cause for concern. Nursing Standard, 25 (38), 28–28.
Lorber, J., & Moore, L. J. (2002). Gender and the social construction of illness (2nd ed.). Lanham, MD: Rowman & Littlefield.
Musto, D. F. (Ed.). (2002). Drugs in America: A documentary history . New York, NY: New York University Press.
Parsons, T. (1951). The social system . New York, NY: Free Press.
Rao, A., & Seaton, M. (2010). The way of boys: Promoting the social and emotional development of young boys . New York, NY: Harper Paperbacks.
Weitz, R. (2013). The sociology of health, illness, and health care: A critical approach (6th ed.). Thousand Oaks, CA: Wadsworth.
Whitehead, K., & Kurz, T. (2008). Saints, sinners and standards of femininity: Discursive constructions of anorexia nervosa and obesity in women’s magazines. Journal of Gender Studies, 17 , 345–358.
Social Problems Copyright © 2015 by University of Minnesota is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
- Fact sheets
- Facts in pictures
Publications
- Questions and answers
- Tools and toolkits
- HIV and AIDS
- Hypertension
- Mental disorders
- Top 10 causes of death
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
- Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Triple Billion
- Data collection tools
- Global Health Observatory
- Insights and visualizations
- COVID excess deaths
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment case
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
- Health topics /
- Social determinants of health
The social determinants of health (SDH) are the non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life. These forces and systems include economic policies and systems, development agendas, social norms, social policies and political systems.
The SDH have an important influence on health inequities - the unfair and avoidable differences in health status seen within and between countries. In countries at all levels of income, health and illness follow a social gradient: the lower the socioeconomic position, the worse the health.
The following list provides examples of the social determinants of health, which can influence health equity in positive and negative ways:
- Income and social protection
- Unemployment and job insecurity
- Working life conditions
- Food insecurity
- Housing, basic amenities and the environment
- Early childhood development
- Social inclusion and non-discrimination
- Structural conflict
- Access to affordable health services of decent quality.
Research shows that the social determinants can be more important than health care or lifestyle choices in influencing health. For example, numerous studies suggest that SDH account for between 30-55% of health outcomes. In addition, estimates show that the contribution of sectors outside health to population health outcomes exceeds the contribution from the health sector.
Addressing SDH appropriately is fundamental for improving health and reducing longstanding inequities in health, which requires action by all sectors and civil society.
There are challenges to overcome in implementing action to address health inequities through the social determinants of health. The social determinants of health equity is a complex and multifaceted field. It involves a wide range of stakeholders within and beyond the health sector and all levels of government. In addition, social determinants of health data can be difficult to collect and share.
While the evidence base on the social determinants of health has strengthened during the past decade, the evidence base on what works needs to be strengthened and good practices disseminated effectively.
Three areas for critical action identified in the report of the Global Commission on Social Determinants of Health reflect their importance in tackling inequities in health. These include:
The circumstances in which people are born, grow, live, work and age;
The structural drivers of those conditions of daily life (for example, macroeconomic and urbanization policies and governance);
Expand the knowledge base, develop a workforce that is trained in the social determinants of health, and raise public awareness about the social determinants of health.
Scaled up and systematic action is required that is universal but proportionate to the disadvantage across the social gradient. This is necessary for effective delivery to addressing inequities in health and promoting healthier populations.
Life expectancy and healthy life expectancy have increased, but unequally. There remain persistent and widening gaps between those with the best and worst health and well-being.
Poorer populations systematically experience worse health than richer populations. For example:
- There is a difference of 18 years of life expectancy between high- and low- income countries;
- In 2016, the majority of the 15 million premature deaths due to non-communicable diseases (NCDs) occurred in low- and middle-income countries;
- Relative gaps within countries between poorer and richer subgroups for diseases like cancer have increased in all regions across the world;
- The under-5 mortality rate is more than eight times higher in Africa than the European region. Within countries, improvements in child health between poorest and richest subgroups have been impaired by slower improvements for poorer subgroups.
Such trends within and between countries are unfair, unjust and avoidable. Many of these health differences are caused by the decision-making processes, policies, social norms and structures which exist at all levels in society.
Inequities in health are socially determined, preventing poorer populations from moving up in society and making the most of their potential.
Pursuing health equity means striving for the highest possible standard of health for all people and giving special attention to the needs of those at greatest risk of poor health, based on social conditions.
Action requires not only equitable access to healthcare but also means working outside the healthcare system to address broader social well-being and development.
“Health equity is defined as the absence of unfair and avoidable or remediable differences in health among population groups defined socially, economically, demographically or geographically”.
- Social determinants of health: Key concepts
- The Global Health Observatory
- Occupational Burden of Disease Application tool
- Special Initiative for Action on the SDH for Advancing Health Equity
- EB148/24 Report by the Director-General
- EB148.R2 Social determinants of health
- WHA65.8 Outcome of the World Conference on Social Determinants of Health (2012)
- WHA62.14 Reducing health inequities through action on the social determinants of health (2009)
WHO releases new guidance on monitoring the social determinants of health equity
WHO launches commission to foster social connection
On World Cities Day 2023, WHO calls for increased financing for a sustainable, healthy urban future for all
On World Cities Day 2022, WHO calls on countries to “Act Local to Go Global”
Building the evidence for action
Promoting Health in All Policies and intersectoral action capacities

Operational framework for monitoring social determinants of health equity
Social determinants of health – broadly defined as the conditions in which people are born, grow, live, work and age, and people’s access to...

Progress report on the United Nations Decade of Healthy Ageing, 2021-2023
The purpose of this report is to: assess the extent of progress made in the first phase of implementation of the UN Decade of Healthy Ageing, ...

Integrating the social determinants of health into health workforce education and training
Social inequalities are perpetuating unhealthy living and working conditions and behaviours. These causes are commonly called ‘the social determinants...

Working together for equity and healthier populations: sustainable multisectoral collaboration based...
This document provides practical advice for implementing multisectoral collaboration for healthy public policies. Health in All Policies (HiAP) approaches...
Social determinants of health discussion paper series
Health in all policies as part of the primary health care agenda on multisectoral action health in all policies as part of the primary health care agenda on multisectoral action, intersectoral factors influencing equity-oriented progress towards universal health coverage: results from a scoping review of literature intersectoral factors influencing equity-oriented progress towards universal health coverage: results from a scoping review of literature, public health agencies and cash transfer programmes: making the case for greater involvement public health agencies and cash transfer programmes: making the case for greater involvement, action on the social determinants of health: learning from previous experiences action on the social determinants of health: learning from previous experiences, a conceptual framework for action on the social determinants of health a conceptual framework for action on the social determinants of health, monitoring social well-being to support policies on the social determinants of health: the case of new zealand's "social reports / te purongo oranga tangata" monitoring social well-being to support policies on the social determinants of health: the case of new zealand's "social reports / te purongo oranga tangata", social determinants of health sectoral briefing series, housing: shared interests in health and development housing: shared interests in health and development, social protection: shared interests in vulnerability reduction and development social protection: shared interests in vulnerability reduction and development, energy: shared interests in sustainable development and energy services energy: shared interests in sustainable development and energy services, education : shared interests in well-being and development education : shared interests in well-being and development, transport (road transport) : shared interests in sustainable outcomes transport (road transport) : shared interests in sustainable outcomes.

Integrating the Social Determinants of Health into Health Workforce Education and Training

The repercussions of COVID-19 will be felt for generations to come: We know what to do
Save the date: 1st Global Ministerial Conference on Ending Violence Against Children
15th World Conference on Injury Prevention and Safety Promotion
Pornography, young people, and the commercial and social determinants of violence
Related links
- Action: SDG
- Bulletin of the World Health Organization (Special theme: social determinants of health)
- Global action on social determinants of health (Bulletin article)
- The need to monitor actions on the social determinants of health (Bulletin article)
- Implementing equity: the Commission on Social Determinants of Health (Bulletin article)
- Health priorities and the social determinants of health (EMRO journal article)
- Economic and social determinants of disease (Bulletin article)
- Impact of non-health policies on infant mortality through the social determinants pathway (Bulletin article)
- Towards social protection for health: an agenda for research and policy in eastern and western Europe
- Inclusive growth as a route to tackling health inequities
- Global Status Report on Health in All Policies
- Global Network for Health in All Policies
- Implications of the Adelaide Statement on Health in All Policies
- The role of parliamentary scrutiny in promoting Health in All Policies
Related health topics
Commercial determinants of health
Environmental health
Urban health
Advertisement
Social Factors of Health Care: a Thematic Analysis of First and Second Year Medical Student Reflections
- Original Research
- Published: 17 August 2021
- Volume 31 , pages 1685–1692, ( 2021 )
Cite this article

- Jacob T. Kirkland 1 ,
- Aiden Berry 2 ,
- Gary L. Beck Dallaghan ORCID: orcid.org/0000-0002-8539-6969 3 ,
- Zach Moore 4 &
- Thomas F. Koonce 5
236 Accesses
15 Altmetric
Explore all metrics
Addressing health disparities is necessary to ensure appropriate care for patients. This study examined the impact of Clinical Week experiences on students’ recognition of social determinants of health early in their medical education.
A 5-day experience each of the first three semesters of medical school provided direct patient care experiences. Two Clinical Weeks were spent in outpatient clinics located primarily in rural areas. Students completed a reflective writing assignment about their experiences after each 5-day experience. Ninety-two reflections during AY 2018–2019 included discussions about social determinants of health. Two investigators analyzed these essays independently using narrative inquiry techniques. After inductive coding was complete, researchers discussed themes and their broader meaning.
Themes emerged related to health disparities experienced by rural communities, minority populations, and both uninsured and underinsured patients. Reflections emphasized a lack of public accommodations in rural settings, such as public transportation and access to healthy food. Students noted how ethnic, cultural, and linguistic identity affect a patient’s experience with healthcare. Other themes involved the challenges patients face affording treatment plans and conversely how health status can impact economic stability. Finally, students emphasized the importance of physician advocacy in overcoming such barriers to quality health care.
Conclusions
Although not the emphasis of Clinical Week, students’ reflections identified critical social issues impacting the health of patients they encountered. This experience could be adapted at other institutions.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

A social ecological approach to promote learning health disparities in the clinical years: impact of a home-visiting educational program for medical students

Enhancing student perspectives of humanism in medicine: reflections from the Kalaupapa service learning project
Cross-cultural perspectives on the patient-provider relationship: a qualitative study exploring reflections from ghanaian medical students following a clinical rotation in the united states, data availability.
Data is available upon request of the corresponding author.
Braveman P, Egerter S, Williams DR. The social determinants of health: coming of age. Ann Rev Pub Health. 2011;32:381–98.
Article Google Scholar
Marmot M. Health in an unequal world. Lancet. 2006;368(9552):2081–94.
Doobay-Persaud A, Adler MD, Bartell TR, et al. Teaching the social determinants of health in undergraduate medical education: a scoping review. J Gen Intern Med. 2019;34(5):720–30.
CDC. Behavioral Risk Factor Surveillance. In: Atlanta, GA: US Department of Health and Human Services; 2019.
Semega J, Kollar M, Creamer J, Mohanty A. Income and poverty in the United States: 2018 In: Bureau USC, editor. Washington, DC: U.S. Census Bureau; 2019.
Skochelak SEHR, Lawson LE, Starr SR, Borkan JM, Gonzalo JD. Health Systems Science. 1st ed. Cambridge, MA: Elsevier; 2016.
Google Scholar
Behforouz HL, Drain PK, Rhatigan JJ. Rethinking the social history. N Engl J Med. 2014;371(14):1277–9.
Classroom to Clinic: First-years in the Field. http://news.unchealthcare.org/som-vital-signs/2016/march-17/2016-clinical-week . Published 2017. Accessed 1 Jul 2020.
Ribeiro LMC, Mamede S, de Brito EM, Moura AS, de Faria RMD, Schmidt HG. Effects of deliberate reflection on students’ engagement in learning and learning outcomes. Med Educ. 2019;53(4):390–7.
Ribeiro LM, Mamede S, Moura AS, de Brito EM, de Faria RM, Schmidt HG. Effect of reflection on medical students’ situational interest: an experimental study. Med Educ. 2018;52(5):488–96.
Burck C. Comparing qualitative research methodologies for systemic research: the use of grounded theory, discourse analysis and narrative analysis. J Fam Therapy. 2005;27(3):237–62.
Thornton RL, Glover CM, Cené CW, Glik DC, Henderson JA, Williams DR. Evaluating strategies for reducing health disparities by addressing the social determinants of health. Health Aff. 2016;35(8):1416–23.
Juckett G, Unger K. Appropriate use of medical interpreters. Amer Fam Phys. 2014;90(7):476–80.
Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255–99.
Bagchi AD, Dale S, Verbitsky-Savitz N, Andrecheck S, Zavotsky K, Eisenstein R. Examining effectiveness of medical interpreters in emergency departments for Spanish-speaking patients with limited English proficiency: results of a randomized controlled trial. Ann Emerg Med. 2011;57(3):248–56. e1-4.
Chaiyachati KH, Shea JA, Asch DA, et al. Assessment of inpatient time allocation among first-year internal medicine residents using time-motion observations. JAMA Int Med. 2019;179(6):760–7.
Powell LM, Slater S, Mirtcheva D, Bao Y, Chaloupka FJ. Food store availability and neighborhood characteristics in the United States. Prevent Med. 2007;44(3):189–95.
Garasky S, Morton LW, Greder KA. The food environment and food insecurity: perceptions of rural, suburban, and urban food pantry clients in Iowa. Fam Econ Nutr Rev. 2004;16(2):41.
Ramirez AS, Rios LKD, Valdez Z, Estrada E, Ruiz A. Bringing produce to the people: implementing a social marketing food access intervention in rural food deserts. J Nutr Educ Behav. 2017;49(2):166–74. e1.
Walker RE, Keane CR, Burke JG. Disparities and access to healthy food in the United States: a review of food deserts literature. Health Place. 2010;16(5):876–84.
Dixon MA, Chartier KG. Alcohol use patterns among urban and rural residents: demographic and social influences. Alcohol Res Health. 2016;38(1):69.
Buettner-Schmidt K, Miller DR, Maack B. Disparities in rural tobacco use, smoke-free policies, and tobacco taxes. West J Nurs Res. 2019;41(8):1184–202.
Hedegaard H, Miniño AM, Warner M. Urban–rural differences in drug overdose death rates, by sex, age, and type of drugs involved, 2017. NCHS Data Brief. 2019;345:1–8.
Cicero TJ, Ellis MS, Surratt HL, Kurtz SP. The changing face of heroin use in the United States: a retrospective analysis of the past 50 years. JAMA Psychiat. 2014;71(7):821–6.
Rural Transportation at a Glance [Brochure]. In: Agriculture USDO, editor. Washington, DC: U.S. Department of Agriculture; 2005.
Smith AS, Trevelyan E. The older population in rural America: 2012–2016 In: Bureau USC, editor. Washington, DC: U.S. Census Bureau; 2019.
Wisnivesky JP, Krauskopf K, Wolf MS, et al. The association between language proficiency and outcomes of elderly patients with asthma. Ann Allerg Asthma Im. 2012;109(3):179–84.
Lindholm M, Hargraves JL, Ferguson WJ, Reed G. Professional language interpretation and inpatient length of stay and readmission rates. J Gen Intern Med. 2012;27(10):1294–9.
Wu MS, Rawal S. “It’s the difference between life and death”: the views of professional medical interpreters on their role in the delivery of safe care to patients with limited English proficiency. PloS One. 2017;12(10). e0185659.
Wasserman M, Renfrew MR, Green AR, et al. Identifying and preventing medical errors in patients with limited English proficiency: key findings and tools for the field. J Healthc Qual. 2014;36(3):5–16.
Johnson K, O’Mahony S, Elk R, Thomson R, Reaves A, Terry A. Improving the care of culturally diverse patients: strategies to address and navigate the elephant in the room (P09). J Pain Symptom Manage. 2019;57(2):357.
Sullivan LS. Trust, risk, and race in American Medicine. Hastings Cent Rep. 2020;50(1):18–26.
Smith SS. Race and trust. Ann Rev Sociol. 2010;36:453–75.
Alsan M, Wanamaker M, Hardeman RR. The Tuskegee study of untreated syphilis: a case study in peripheral trauma with implications for health professionals. J Gen Intern Med. 2020;35(1):322–5.
Pergolotti M, Lavery J, Reeve BB, Dusetzina SB. Therapy caps and variation in cost of outpatient occupational therapy by provider, insurance status, and geographic region. Am J Occup Ther. 2018;72(2):7202205050p1–9.
Niedzwiecki MJ, Hsia RY, Shen YC. Not all insurance is equal: differential treatment and health outcomes by insurance coverage among nonelderly adult patients with heart attack. J Am Heart Assoc. 2018;7(11):e008152.
Chambers J, Pope E, Bungay K, et al. A comparison of coverage restrictions for biopharmaceuticals and medical procedures. Value Health. 2018;21(4):400–6.
Health HTHCSoP. Life experiences and income inequality in the United States; 2020.
Silvaggi F, Leonardi M, Guastafierro E, et al. Chronic diseases & employment: an overview of existing training tools for employers. Int J Environ Res Public Health. 2019;16(5):718.
Barra L, Borchin R, Burroughs C, et al. Impact of vasculitis on employment and income. Clin Exp Rheumatol. 2018;36(Suppl 111):58.
Alexander GC, Casalino LP, Meltzer DO. Patient-physician communication about out-of-pocket costs. JAMA. 2003;290(7):953–8.
Ubel PA, Zhang CJ, Hesson A, et al. Study of physician and patient communication identifies missed opportunities to help reduce patients’ out-of-pocket spending. Health Aff. 2016;35(4):654–61.
Hunter WG, Hesson A, Davis JK, et al. Patient-physician discussions about costs: definitions and impact on cost conversation incidence estimates. BMC Health Serv Res. 2016;16(1):108.
Smith GD, Bartley M, Blane D. The Black report on socioeconomic inequalities in health 10 years on. BMJ-British Medical Journal. 1990;301(6748):373.
Harper S, Lynch J. Trends in socioeconomic inequalities in adult health behaviors among US states, 1990–2004. Public Health Rep. 2007;122(2):177–89.
Wang J, Geng L. Effects of socioeconomic status on physical and psychological health: lifestyle as a mediator. Int J Environ Res Public Health. 2019;16(2):281.
Download references
Author information
Authors and affiliations.
University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Jacob T. Kirkland
Department of Medicine-Pediatrics, University of Michigan Medical Center, Ann Arbor, MI, USA
Aiden Berry
Office of Educational Scholarship, University of North Carolina School of Medicine, Chapel Hill, NC, USA
Gary L. Beck Dallaghan
Office of Academic Affairs, University of North Carolina Adams School of Dentistry, Chapel Hill, NC, USA
Department of Family Medicine, University of North Carolina School of Medicine, Chapel Hill, NC, USA
Thomas F. Koonce
You can also search for this author in PubMed Google Scholar
Contributions
Each of the authors contributed to conception of this study and participated in the analysis of the data. Each author contributed to the manuscript and has given approval for the final version submitted.
Corresponding author
Correspondence to Gary L. Beck Dallaghan .
Ethics declarations
Ethics approval.
This study was reviewed and approved by the institutional review board as exempt.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Reprints and permissions
About this article
Kirkland, J.T., Berry, A., Beck Dallaghan, G.L. et al. Social Factors of Health Care: a Thematic Analysis of First and Second Year Medical Student Reflections. Med.Sci.Educ. 31 , 1685–1692 (2021). https://doi.org/10.1007/s40670-021-01360-5
Download citation
Accepted : 20 July 2021
Published : 17 August 2021
Issue Date : October 2021
DOI : https://doi.org/10.1007/s40670-021-01360-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Medical student
- Social determinants of health
- Pre-clinical education
- Reflective writing
- Find a journal
- Publish with us
- Track your research
Albert Bandura’s Social Cognitive Theory
Charlotte Nickerson
Research Assistant at Harvard University
Undergraduate at Harvard University
Charlotte Nickerson is a student at Harvard University obsessed with the intersection of mental health, productivity, and design.
Learn about our Editorial Process
Saul Mcleod, PhD
Editor-in-Chief for Simply Psychology
BSc (Hons) Psychology, MRes, PhD, University of Manchester
Saul Mcleod, PhD., is a qualified psychology teacher with over 18 years of experience in further and higher education. He has been published in peer-reviewed journals, including the Journal of Clinical Psychology.
Olivia Guy-Evans, MSc
Associate Editor for Simply Psychology
BSc (Hons) Psychology, MSc Psychology of Education
Olivia Guy-Evans is a writer and associate editor for Simply Psychology. She has previously worked in healthcare and educational sectors.
On This Page:
Key Takeaways
- Social cognitive theory emphasizes the learning that occurs within a social context. In this view, people are active agents who can both influence and are influenced by their environment.
- The theory was founded most prominently by Albert Bandura, who is also known for his work on observational learning, self-efficacy, and reciprocal determinism.
- One assumption of social learning is that we learn new behaviors by observing the behavior of others and the consequences of their behavior.
- If the behavior is rewarded (positive or negative reinforcement), we are likely to imitate it; however, if the behavior is punished, imitation is less likely. For example, in Bandura and Walters’ experiment, the children imitated more the aggressive behavior of the model who was praised for being aggressive to the Bobo doll.
- Social cognitive theory has been used to explain a wide range of human behavior, ranging from positive to negative social behaviors such as aggression, substance abuse, and mental health problems.

How We Learn From the Behavior of Others
Social cognitive theory views people as active agents who can both influence and are influenced by their environment.
The theory is an extension of social learning that includes the effects of cognitive processes — such as conceptions, judgment, and motivation — on an individual’s behavior and on the environment that influences them.
Rather than passively absorbing knowledge from environmental inputs, social cognitive theory argues that people actively influence their learning by interpreting the outcomes of their actions, which, in turn, affects their environments and personal factors, informing and altering subsequent behavior (Schunk, 2012).
By including thought processes in human psychology, social cognitive theory is able to avoid the assumption made by radical behaviorism that all human behavior is learned through trial and error. Instead, Bandura highlights the role of observational learning and imitation in human behavior.
Numerous psychologists, such as Julian Rotter and the American personality psychologist Walter Mischel, have proposed different social-cognitive perspectives.
Albert Bandura (1989) introduced the most prominent perspective on social cognitive theory.
Bandura’s perspective has been applied to a wide range of topics, such as personality development and functioning, the understanding and treatment of psychological disorders, organizational training programs, education, health promotion strategies, advertising and marketing, and more.
The central tenet of Bandura’s social-cognitive theory is that people seek to develop a sense of agency and exert control over the important events in their lives.
This sense of agency and control is affected by factors such as self-efficacy, outcome expectations, goals, and self-evaluation (Schunk, 2012).
Origins: The Bobo Doll Experiments
Social cognitive theory can trace its origins to Bandura and his colleagues, in particular, a series of well-known studies on observational learning known as the Bobo Doll experiments .

In these experiments, researchers exposed young, preschool-aged children to videos of an adult acting violently toward a large, inflatable doll.
This aggressive behavior included verbal insults and physical violence, such as slapping and punching. At the end of the video, the children either witnessed the aggressor being rewarded, or punished or received no consequences for his behavior (Schunk, 2012).
After being exposed to this model, the children were placed in a room where they were given the same inflatable Bobo doll.
The researchers found that those who had watched the model either received positive reinforcement or no consequences for attacking the doll were more likely to show aggressive behavior toward the doll (Schunk, 2012).
This experiment was notable for being one that introduced the concept of observational learning to humans.
Bandura’s ideas about observational learning were in stark contrast to those of previous behaviorists, such as B.F. Skinner.
According to Skinner (1950), learning can only be achieved through individual action.
However, Bandura claimed that people and animals can also learn by watching and imitating the models they encounter in their environment, enabling them to acquire information more quickly.
Observational Learning
Bandura agreed with the behaviorists that behavior is learned through experience. However, he proposed a different mechanism than conditioning.
He argued that we learn through observation and imitation of others’ behavior.
This theory focuses not only on the behavior itself but also on the mental processes involved in learning, so it is not a pure behaviorist theory.

Stages of the Social Learning Theory (SLT)
Not all observed behaviors are learned effectively. There are several factors involving both the model and the observer that determine whether or not a behavior is learned. These include attention, retention, motor reproduction, and motivation (Bandura & Walters, 1963).
The individual needs to pay attention to the behavior and its consequences and form a mental representation of the behavior. Some of the things that influence attention involve characteristics of the model.
This means that the model must be salient or noticeable. If the model is attractive, prestigious, or appears to be particularly competent, you will pay more attention. And if the model seems more like yourself, you pay more attention.
Storing the observed behavior in LTM where it can stay for a long period of time. Imitation is not always immediate. This process is often mediated by symbols. Symbols are “anything that stands for something else” (Bandura, 1998).
They can be words, pictures, or even gestures. For symbols to be effective, they must be related to the behavior being learned and must be understood by the observer.
Motor Reproduction
The individual must be able (have the ability and skills) to physically reproduce the observed behavior. This means that the behavior must be within their capability. If it is not, they will not be able to learn it (Bandura, 1998).
The observer must be motivated to perform the behavior. This motivation can come from a variety of sources, such as a desire to achieve a goal or avoid punishment.
Bandura (1977) proposed that motivation has three main components: expectancy, value, and affective reaction. Firstly, expectancy refers to the belief that one can successfully perform the behavior. Secondly, value refers to the importance of the goal that the behavior is meant to achieve.
The last of these, Affective reaction, refers to the emotions associated with the behavior.
If behavior is associated with positive emotions, it is more likely to be learned than a behavior associated with negative emotions. Reinforcement and punishment each play an important role in motivation.
Individuals must expect to receive the same positive reinforcement (vicarious reinforcement) for imitating the observed behavior that they have seen the model receiving.
Imitation is more likely to occur if the model (the person who performs the behavior) is positively reinforced. This is called vicarious reinforcement.
Imitation is also more likely if we identify with the model. We see them as sharing some characteristics with us, i.e., similar age, gender, and social status, as we identify with them.
Features of Social Cognitive Theory
The goal of social cognitive theory is to explain how people regulate their behavior through control and reinforcement in order to achieve goal-directed behavior that can be maintained over time.
Bandura, in his original formulation of the related social learning theory, included five constructs, adding self-efficacy to his final social cognitive theory (Bandura, 1986).
Reciprocal Determinism
Reciprocal determinism is the central concept of social cognitive theory and refers to the dynamic and reciprocal interaction of people — individuals with a set of learned experiences — the environment, external social context, and behavior — the response to stimuli to achieve goals.
Its main tenet is that people seek to develop a sense of agency and exert control over the important events in their lives.
This sense of agency and control is affected by factors such as self-efficacy, outcome expectations, goals, and self-evaluation (Bandura, 1989).
To illustrate the concept of reciprocal determinism, Consider A student who believes they have the ability to succeed on an exam (self-efficacy) is more likely to put forth the necessary effort to study (behavior).
If they do not believe they can pass the exam, they are less likely to study. As a result, their beliefs about their abilities (self-efficacy) will be affirmed or disconfirmed by their actual performance on the exam (outcome).
This, in turn, will affect future beliefs and behavior. If the student passes the exam, they are likely to believe they can do well on future exams and put forth the effort to study.
If they fail, they may doubt their abilities (Bandura, 1989).
Behavioral Capability
Behavioral capability, meanwhile, refers to a person’s ability to perform a behavior by means of using their own knowledge and skills.
That is to say, in order to carry out any behavior, a person must know what to do and how to do it. People learn from the consequences of their behavior, further affecting the environment in which they live (Bandura, 1989).
Reinforcements
Reinforcements refer to the internal or external responses to a person’s behavior that affect the likelihood of continuing or discontinuing the behavior.
These reinforcements can be self-initiated or in one’s environment either positive or negative. Positive reinforcements increase the likelihood of a behavior being repeated, while negative reinforcers decrease the likelihood of a behavior being repeated.
Reinforcements can also be either direct or indirect. Direct reinforcements are an immediate consequence of a behavior that affects its likelihood, such as getting a paycheck for working (positive reinforcement).
Indirect reinforcements are not immediate consequences of behavior but may affect its likelihood in the future, such as studying hard in school to get into a good college (positive reinforcement) (Bandura, 1989).
Expectations
Expectations, meanwhile, refer to the anticipated consequences that a person has of their behavior.
Outcome expectations, for example, could relate to the consequences that someone foresees an action having on their health.
As people anticipate the consequences of their actions before engaging in a behavior, these expectations can influence whether or not someone completes the behavior successfully (Bandura, 1989).
Expectations largely come from someone’s previous experience. Nonetheless, expectancies also focus on the value that is placed on the outcome, something that is subjective from individual to individual.
For example, a student who may not be motivated to achieve high grades may place a lower value on taking the steps necessary to achieve them than someone who strives to be a high performer.
Self-Efficacy
Self-efficacy refers to the level of a person’s confidence in their ability to successfully perform a behavior.
Self-efficacy is influenced by a person’s own capabilities as well as other individual and environmental factors.
These factors are called barriers and facilitators (Bandura, 1989). Self-efficacy is often said to be task-specific, meaning that people can feel confident in their ability to perform one task but not another.
For example, a student may feel confident in their ability to do well on an exam but not feel as confident in their ability to make friends.
This is because self-efficacy is based on past experience and beliefs. If a student has never made friends before, they are less likely to believe that they will do so in the future.
Modeling Media and Social Cognitive Theory
Learning would be both laborious and hazardous in a world that relied exclusively on direct experience.
Social modeling provides a way for people to observe the successes and failures of others with little or no risk.
This modeling can take place on a massive scale. Modeling media is defined as “any type of mass communication—television, movies, magazines, music, etc.—that serves as a model for observing and imitating behavior” (Bandura, 1998).
In other words, it is a means by which people can learn new behaviors. Modeling media is often used in the fashion and taste industries to influence the behavior of consumers.
This is because modeling provides a reference point for observers to imitate. When done effectively, modeling can prompt individuals to adopt certain behaviors that they may not have otherwise engaged in.
Additionally, modeling media can provide reinforcement for desired behaviors.
For example, if someone sees a model wearing a certain type of clothing and receives compliments for doing so themselves, they may be more likely to purchase clothing like that of the model.
Observational Learning Examples
There are numerous examples of observational learning in everyday life for people of all ages.
Nonetheless, observational learning is especially prevalent in the socialization of children. For example:
- A newer employee avoids being late to work after seeing a colleague be fired for being late.
- A new store customer learns the process of lining up and checking out by watching other customers.
- A traveler to a foreign country learning how to buy a ticket for a train and enter the gates by witnessing others do the same.
- A customer in a clothing store learns the procedure for trying on clothes by watching others.
- A person in a coffee shop learns where to find cream and sugar by watching other coffee drinkers locate the area.
- A new car salesperson learning how to approach potential customers by watching others.
- Someone moving to a new climate and learning how to properly remove snow from his car and driveway by seeing his neighbors do the same.
- A tenant learning to pay rent on time as a result of seeing a neighbor evicted for late payment.
- An inexperienced salesperson becomes successful at a sales meeting or in giving a presentation after observing the behaviors and statements of other salespeople.
- A viewer watches an online video to learn how to contour and shape their eyebrows and then goes to the store to do so themselves.
- Drivers slow down after seeing that another driver has been pulled over by a police officer.
- A bank teller watches their more efficient colleague in order to learn a more efficient way of counting money.
- A shy party guest watching someone more popular talk to different people in the crowd, later allowing them to do the same thing.
- Adult children behave in the same way that their parents did when they were young.
- A lost student navigating a school campus after seeing others do it on their own.
Social Learning vs. Social Cognitive Theory
Social learning theory and Social Cognitive Theory are both theories of learning that place an emphasis on the role of observational learning.
However, there are several key differences between the two theories. Social learning theory focuses on the idea of reinforcement, while Social Cognitive Theory emphasizes the role of cognitive processes.
Additionally, social learning theory posits that all behavior is learned through observation, while Social Cognitive Theory allows for the possibility of learning through other means, such as direct experience.
Finally, social learning theory focuses on individualistic learning, while Social Cognitive Theory takes a more holistic view, acknowledging the importance of environmental factors.
Though they are similar in many ways, the differences between social learning theory and Social Cognitive Theory are important to understand. These theories provide different frameworks for understanding how learning takes place.
As such, they have different implications in all facets of their applications (Reed et al., 2010).
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory . Prentice-Hall, Inc.
Bandura, A. (1977). Social learning theory . Englewood Cliffs, NJ: Prentice Hall.
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change. Psychological Review, 84 (2), 191.
Bandura, A. (1986). Fearful expectations and avoidant actions as coeffects of perceived self-inefficacy.
Bandura, A. (1989). Human agency in social cognitive theory. American psychologist, 44 (9), 1175.
Bandura, A. (1998). Health promotion from the perspective of social cognitive theory. Psychology and health, 13 (4), 623-649.
Bandura, A. (2003). Social cognitive theory for personal and social change by enabling media. In Entertainment-education and social change (pp. 97-118). Routledge.
Bandura, A. Ross, D., & Ross, S. A. (1961). Transmission of aggression through the imitation of aggressive models. Journal of Abnormal and Social Psychology , 63, 575-582.
LaMort, W. (2019). The Social Cognitive Theory. Boston University.
Reed, M. S., Evely, A. C., Cundill, G., Fazey, I., Glass, J., Laing, A., … & Stringer, L. C. (2010). What is social learning?. Ecology and society, 15 (4).
Schunk, D. H. (2012). Social cognitive theory .
Skinner, B. F. (1950). Are theories of learning necessary?. Psychological Review, 57 (4), 193.
Related Articles

Learning Theories
Aversion Therapy & Examples of Aversive Conditioning
Learning Theories , Psychology , Social Science
Albert Bandura’s Social Learning Theory

Learning Theories , Psychology
Behaviorism In Psychology
Famous Experiments , Learning Theories
Bandura’s Bobo Doll Experiment on Social Learning

Bloom’s Taxonomy of Learning

Child Psychology , Learning Theories
Jerome Bruner’s Theory Of Learning And Cognitive Development
Advertisement
Pre-Exposure Prophylaxis (PrEP)
Social determinants of health (sdoh).
Social determinants of health are the conditions in which we live, learn, work, and play. These conditions can influence the health and well-being of you and y…
Name (required)
Mail (will not be published) (required)
Gimme a site! Just a username, please.
Remember Me
Social Determinants of Health
Essential Information | Doctors’ Note | At-A-Glance Guides | More Resources
Social Determinants of Health (SDOH): A Brief Overview
There are many factors that influence our health. These factors are referred to as determinants of health. One kind of determinant of health is what is in our genes and our biology. Another determinant is our individual behavior, which include choices we make, such as smoking, exercise habits, or the types of foods we eat. A third determinant of our health is a wider set of influences (forces and systems) that shape the conditions of daily life.
SDOH Essential Information
Social determinants of health are the conditions in which we live, learn, work, and play. These conditions can influence the health and well-being of you and your community.
Read Article

SDOH Doctors’ Notes

Doctors’ Notes: What are social determinants of health?
It is important to understand and discuss the non-medical factors that play a role in your short-term and long-term health.
SDOH At-A-Glance Guides

Additional SDOH Resources
Centers for Disease Control and Prevention: Social Determinants of Health
Healthy People 2030: Social Determinants of Health
familydoctor.org is powered by

Visit our interactive symptom checker
The independent source for health policy research, polling, and news.
Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them
Latoya Hill , Samantha Artiga , and Usha Ranji Published: Nov 01, 2022
Stark racial disparities in maternal and infant health in the U.S. have persisted for decades despite continued advancements in medical care. The disparate impact of the COVID-19 pandemic for people of color has brought a new focus to health disparities, including the longstanding inequities in maternal and infant health. Additionally, with Roe v. Wade now overturned, increased barriers to abortion for people of color may widen the already existing large disparities in maternal and infant health. Recently, there has been increased attention and focus on improving maternal and infant health and reducing disparities in these areas, including a range of efforts at the federal level. This brief provides an overview of racial disparities for selected measures of maternal and infant health, discusses the factors that drive these disparities, and provides an overview of recent efforts to address them. 1 It finds:
Black and American Indian and Alaska Native (AIAN) women have higher rates of pregnancy-related death compared to White women. Pregnancy-related mortality rates among Black and AIAN women are over three and two times higher, respectively, compared to the rate for White women (41.4 and 26.2 vs. 13.7 per 100,000). Black, AIAN, and Native Hawaiian and Other Pacific Islander (NHOPI) women also have higher shares of preterm births, low birthweight births, or births for which they received late or no prenatal care compared to White women. Infants born to Black, AIAN, and NHOPI people have markedly higher mortality rates than those born to White women. Maternal death rates increased during the COVID-19 pandemic and racial disparities widened for Black women.
Maternal and infant health disparities are symptoms of broader underlying social and economic inequities that are rooted in racism and discrimination. Differences in health insurance coverage and access to care play a role in driving worse maternal and infant health outcomes for people of color. However, inequities in broader social and economic factors and structural and systemic racism and discrimination are primary drivers for maternal and infant health. Notably, disparities in maternal and infant health persist even when controlling for certain underlying social and economic factors, such as education and income, pointing to the roles racism and discrimination play in driving disparities.
The increased awareness and attention to maternal and infant health have contributed to a rise in efforts and resources focused on improving health outcomes in these areas and reducing disparities. These include efforts to expand access to coverage and care, increase access to a broader array of services and providers that support maternal and infant health, diversity the health care workforce, and enhance data collection and reporting. However, addressing social and economic factors that contribute to poorer health outcomes and disparities will also be important. Moreover, the persistence of disparities in maternal health across income and education levels, points to the importance of addressing the roles of racism and discrimination within the health care system as part of efforts to improve health and advance equity.
Introduction
The COVID-19 pandemic has exacerbated longstanding disparities in health and health care for people of color, including stark disparities in maternal and infant health. Despite continued advancements in medical care, rates of maternal mortality and morbidity and pre-term birth have been rising in the U.S. Maternal and infant mortality rates in the U.S. are far higher than those in similarly large and wealthy countries, and people of color are at increased risk for poor maternal and infant health outcomes compared to their White peers. Amid the COVID-19 pandemic, maternal deaths have continued to rise and racial disparities have further widened. Moreover, with the overturning of Roe v. Wade , increased barriers to abortion for people of color may widen the already existing large disparities in maternal and infant health. Together these factors have contributed to growing attention and efforts to improve overall maternal and infant health and reduce disparities in these areas.
This issue brief provides analysis of racial and ethnic disparities across selected measures of maternal and infant health, discusses the factors that drive these disparities, and provides an overview of recent efforts to address them. It is based on KFF analysis of publicly available data from CDC WONDER online database, the National Center for Health Statistics (NCHS) National Vital Statistics Reports, CDC Pregnancy Mortality Surveillance System, and a report from the US Government Accountability Office (GAO). While this brief focuses on racial/ethnic disparities in maternal and infant health, wide disparities also exist across other dimensions; for example, there is significant variation in some of these measures across states and disparities within rural communities.
Status of Racial Disparities in Maternal and Infant Health
Pregnancy-related mortality rates.
Approximately 700 women die in the U.S. each year as a result of pregnancy or its complications. Pregnancy-related deaths are deaths that occur within one year of pregnancy. Approximately one third (31%) occur during pregnancy, another third (36%) occur during labor or within the first week postpartum, and the remaining third (33%) occur one week to one year postpartum, underscoring the importance of access to health care beyond the period of pregnancy. Recent data has found that more than eight out of ten (84%) pregnancy-related deaths are preventable. Although leading causes of pregnancy-related death vary by race and ethnicity, cardiovascular conditions are the leading cause of pregnancy-related death among women overall, highlighting the importance of care for chronic conditions on pregnancy-related outcomes. More recent data from detailed maternal mortality reviews in 36 states found mental health conditions to be the overall leading cause of pregnancy related deaths.
Black and AIAN women have pregnancy-related mortality rates that are about three and two times higher, respectively, compared to the rate for White women (41.4 and 26.5 vs. 13.7 per 100,000 live births) (Figure 1). These disparities increase by maternal age. For example, the pregnancy-related mortality rate for Black women between ages 30 to 34 widens to over four times higher than the rate for White women (48.6 vs. 11.3 per 100,000), while the rate for AIAN women in the same age group is nearly four times as high as the rate for White women (41.2 per 100,000). Moreover, they persist across education levels. Notably, the pregnancy-related mortality rate for Black women who completed college education or higher is 5.2 times higher than the rate for White women with the same educational attainment and 1.6 times higher than the rate for White women with less than a high school diploma . There are small differences in the rate pregnancy-related death between Asian and Pacific Islander and White women (14.1 vs. 13.7 per 100,000), and the rate for Hispanic women is lower compared to that of White women (11.2 vs. 13.7 per 100,000). These findings may mask underlying differences in subgroups of these populations. Other research also shows that Black women are at significantly higher risk for severe maternal morbidity , such as preeclampsia , which is significantly more common than maternal death. Further, Black women have higher rates of admission to the intensive care unit during delivery compared to White women, which is considered a marker for severe maternal morbidity.
Maternal death rates increased during the COVID-19 pandemic and racial disparities widened for Black women . According to recent GAO analysis that examined maternal deaths during pregnancy or within 42 days of pregnancy, Black women had the highest maternal mortality rates across racial and ethnic groups during the pandemic in 2020 and 2021 and also experienced the largest increase when compared to the year before the pandemic in 2019 (Figure 2). The maternal mortality rate for Hispanic women was less than the rate for White women prior to the pandemic but increased significantly and was similar to the rate for White women in 2020 and 2021. Data show that most of the increase in maternal deaths in 2020 and all of the increase in 2021 can be attributed to COVID-19 related deaths, which were higher among Black and Hispanic women (13.2 and 8.9 per 100,000, respectively) compared to White women (4.5 per 100,000).
Birth Risks and Outcomes
Black, AIAN, and NHOPI women are more likely than White women to have certain birth risk factors that contribute to infant mortality and can have long-term consequences for the physical and cognitive health of children. Preterm birth (birth before 37 weeks gestation) and low birthweight (defined as a baby born less than 5.5 pounds) are some of the leading causes for infant mortality. Receiving pregnancy-related care late in a pregnancy (defined as starting in the third trimester) or not receiving any pregnancy-related care at all can also increase risk of pregnancy complications. Black, AIAN, and NHOPI women have higher shares of preterm births, low birthweight births, or births for which they received late or no prenatal care compared to White women (Figure 3). Notably, NHOPI women are four times more likely than White women to begin receiving prenatal care in the third trimester or to receive no prenatal care at all (19% vs. 5%). Black women also are nearly twice as likely compared to White women to have a birth with late or no prenatal care compared to White women (9% vs. 5%).
While teen birth rates overall have declined over time, they are higher among Black, Hispanic, AIAN, and NHOPI teens compared to their White counterparts (Figure 4). In contrast, the birth rate among Asian teens is lower than the rate for White teens. Many teen pregnancies are unplanned, and pregnant teens may be less likely to receive early and regular prenatal care. Teen pregnancy also is associated with increased risk of complications during pregnancy and delivery, including preterm birth. Teen pregnancy and childbirth can also have social and economic impacts on teen parents and their children, including disrupting educational completion for the parents and lower school achievement for the children. The drivers of teen pregnancy are multi-faceted and include poverty, history of adverse childhood events, and access to comprehensive education and health care services. Research studies have found that increased use of contraception as well as support for comprehensive sex education have helped lower the rate of teen births nationally.
Reflecting these increased risk factors, infants born to women of color are at higher risk for mortality compared to those born to White women. Infant mortality is defined as the death of an infant within the first year of life, but most cases occur within the first month after birth. The primary causes of infant mortality are birth defects, preterm birth and low birthweight, maternal pregnancy complications, sudden infant death syndrome, and injuries. Infants born to Black women are over twice as likely to die relative to those born to White women (10.4 vs. 4.4 per 1,000), and the mortality rate for infants born to AIAN and NHOPI women (7.7 and 7.2 per 1,000) is nearly twice as high (Figure 5). The mortality rate for infants born to Hispanic mothers is similar to the rate for those born to White women (4.7 vs. 4.4 per 1,000), while infants born to Asian women have a lower mortality rate (3.1 per 1,000). Data also show that fetal death or stillbirths —that is, pregnancy loss after 20-week gestation—are more common among Black women compared to White and Hispanic women. Moreover, causes of stillbirth vary by race and ethnicity, with higher rates of stillbirth attributed to diabetes and maternal complications among Black women compared to White women.
Factors Driving Disparities in Maternal and Infant Health
The factors driving disparities in maternal and infant health are complex and multifactorial. They include differences in health insurance coverage and access to care. However, broader social and economic factors and structural and systemic racism and discrimination, also play a major role (Figure 6). In maternal and infant health specifically, the intersection of race, gender, poverty, and other social factors shapes individuals’ experiences and outcomes. Recently there has been broader recognition of the principles of reproductive justice , which emphasize the role that the social determinants of health and other factors play in reproductive health for communities of color. Notably, Hispanic women and infants fare similarly to their White counterparts on many measures of maternal and infant health despite experiencing increased access barriers and social and economic challenges typically associated with poorer health outcomes. Research suggests that this finding, sometimes referred to as the Hispanic or Latino health paradox , in part, stems from variation in outcomes among subgroups of Hispanic people by origin, nativity, and race, with better outcomes for some groups, particularly recent immigrants to the U.S. However, the findings still are not fully understood.
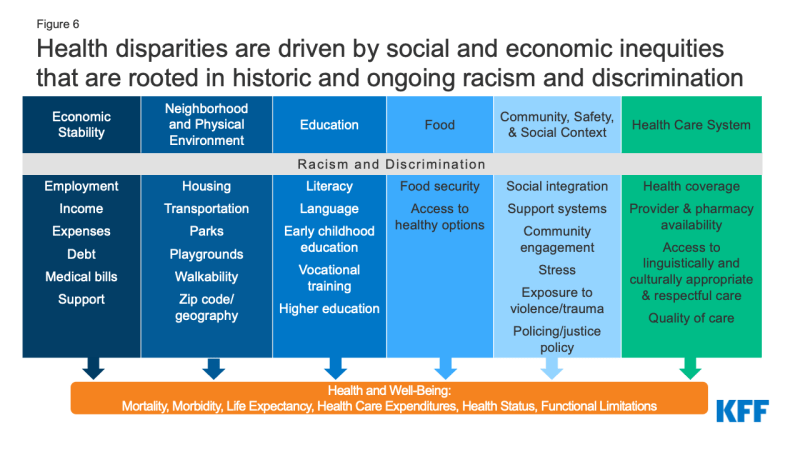
Figure 6: Health disparities are driven by social and economic inequities that are rooted in historic and ongoing racism and discrimination
Disparities in maternal and infant health, in part, reflect increased barriers to care for people of color. Research shows that coverage before, during, and after pregnancy facilitates access to care that supports healthy pregnancies, as well as positive maternal and infant outcomes after childbirth. Overall, people of color are more likely to be uninsured and face other barriers to care . Medicaid helps to fill these coverage gaps during pregnancy and for children. However, women of color are at increased risk of being uninsured prior to their pregnancy and, historically, many have lost coverage at the end of the 60-day Medicaid postpartum coverage period due to lower eligibility levels for parents compared to pregnant women, particularly in states that have not implemented the Affordable Care Act (ACA) Medicaid expansion. Beyond health coverage, people of color face other increased barriers to care , including limited access to providers and hospitals and lack of access to culturally and linguistically appropriate care. These challenges may be particularly pronounced in rural and medically underserved areas. For example, research suggests that a rise in closures of hospitals and obstetric units in rural areas has a disproportionate impact in communities with larger shares of Black patients.
Research also highlights the role of racism and discrimination plays in driving racial disparities in maternal and infant health . Research has documented that social and economic factors, racism , and chronic stress contribute to poor maternal and infant health outcomes, including higher rates of perinatal depression and preterm birth among African American women and higher rates of mortality among Black infants. In recent years, research and news reports have raised attention to the effects of provider discrimination during pregnancy and delivery. News reporting and maternal mortality case reviews have called attention to a number of maternal deaths and near misses among women of color where providers did not or were slow to listen to patients. In one study , Indigenous, Hispanic, and Black women reported significantly higher rates of mistreatment (such as shouting and scolding, ignoring or refusing requests for help) during the course of their pregnancy. Even controlling for insurance status, income, age, and severity of conditions, people of color are less likely to receive routine medical procedures and experience a lower quality of care . One recent study of hospital births in Florida found that there were significant improvements in mortality for Black newborns who were cared for by Black physicians, pointing to the importance of culturally concordant or competent care. A KFF/The Undefeated survey found that most Black adults believe the health care system treats people unfairly based on their race, and one in five Black and Hispanic adults report they were personally treated unfairly because of their race or ethnicity while getting health care in the past year, with a higher share of Black mothers reporting unfair treatment. Black adults also were more likely than White adults to report feeling a provider didn’t believe they were telling the truth and being refused a test, treatment, or pain medication they thought they needed.
Current Efforts to Address Maternal and Infant Health Disparities
Increased awareness and attention to maternal and infant health have contributed to a rise in efforts and resources focused on improving maternal health and infant health outcomes and reducing disparities. These include efforts to expand access to coverage and care, increase access to a broader array of services and providers that support maternal and infant health, diversity the health care workforce, and enhance data collection and reporting.
In June 2022, the Biden Administration released the Blueprint for Addressing the Maternal Health Crisis . The Blueprint outlines priorities and actions across federal agencies to improve access to coverage and care, expand and enhance data collection and research, grow, and diversify the perinatal workforce, strengthen social and economic support, and increase trainings and incentives to support women being active participants in their care before, during and after pregnancy. Several of these proposals are included in the MOMNIBUS, a federal legislative package sponsored by the Congressional Black Maternal Health Caucus. Federal agencies also have announced plans and actions to support the Blueprint, including the Centers for Medicare & Medicaid Services (CMS), which released a maternity care action plan in July 2022; the Health Resources and Services Administration (HRSA), which has committed $350 million to states to strengthen maternal and child health, and the Office of the Assistant Secretary for Health (OASH), which invested $8.5 million in initiatives designed to reduce pregnancy-related deaths and complications that disproportionately impact people of color and those living in rural areas.
Recent federal legislation has expanded access to and helped stabilize Medicaid coverage during the postpartum period. Medicaid covers almost half of births nationally. However, historically, many pregnant women lost coverage at the end of a 60-day postpartum coverage period because eligibility levels are lower for parents than pregnant women in many states, particularly those that have not implemented the Affordable Care Act (ACA) Medicaid expansion. The American Rescue Plan Act (ARPA) of 2021 provided states a new option for five years, beginning April 1, 2022, to extend postpartum coverage to a full year. As of October 27, 2022, 27 states, including DC, had implemented a 12-month postpartum coverage extension , and an additional seven states were planning to implement the extension. KFF analysis suggests that the coverage extension could prevent hundreds of thousands of enrollees from losing coverage in the months after delivery. In addition, at the start of the pandemic, Congress enacted the Families First Coronavirus Response Act (FFCRA), which included a requirement that Medicaid programs keep people continuously enrolled through the end of the month in which the COVID-19 PHE ends in exchange for enhanced federal funding. This provision has prevented coverage gaps or losses that otherwise might have occurred during the postpartum period due to changes in eligibility and/or administrative challenges associated with maintaining coverage. However, coverage losses may occur after states resume redeterminations of eligibility when the PHE ends. Additional actions may also help to reduce disparities , including adoption of the ACA Medicaid expansion in the 12 remaining states that have not yet expanded, as nearly six in ten adults in the coverage gap in these states are adults of color. Further, Medicaid expansion promotes continuity of coverage in the prenatal and postpartum periods. The Biden Administration Blueprint encourages states to take-up the ARPA postpartum coverage option and urges Congress to close the Medicaid coverage gap and require all states to provide 12 months postpartum Medicaid and CHIP coverage.
Implementation of evidence-based best practices may help to improve maternal and infant health outcomes. As part of its maternity care action plan, CMS has outlined a proposal for a “Birthing-Friendly” hospital designation that would provide public information on hospitals that have implemented best practices in areas of health care quality, safety, and equity for pregnant and postpartum patients. Moreover, in 2022, CMS has launched a new effort within its maternal and infant health initiative to reduce low-risk Cesarean births to improve infant and maternal health. This program is centered around a learning collaborative that outlines approaches Medicaid and CHIP agencies can put in place to reduce low-risk cesarean deliveries and works directly with states to implement evidence-based best practices in their state.
Recent actions have enhanced access to data on maternal and infant health outcomes and disparities. For example, the Centers for Disease Control and Prevention (CDC) conducts national pregnancy-related mortality surveillance and regularly releases findings as a source of information around the risk factors and causes of pregnancy-related deaths. The CDC also developed Levels of Care Assessment Tool (LOCATe) to assist states by standardizing their assessments of levels of maternal and neonatal care and promotes the Hear Her campaign to raise awareness of urgent maternal warning signs during and after pregnancy. In addition, the CDC supports state efforts to prevent maternal deaths through several efforts including the Enhancing Reviews and Surveillance to Eliminate Maternal Mortality (ERASE MM) program and perinatal quality collaboratives (PQCs), which aide in increasing understanding of the drivers of pregnancy related mortality and identify health care processes that contribute to improved outcomes for mothers and infants to reduce racial disparities and geographic disparities. Maternal mortality review committees in several states are comprised of clinicians, community members, researchers, and other experts to review all deaths within one year of pregnancy, and identify causes, drivers, and opportunities for quality improvement. Data collection by these committees has been particularly important in understanding that a large share of deaths are preventable as well as identifying the significant portion of deaths that occur after delivery and encouraging efforts to strengthen care in the postpartum period. Moreover, there are several research and data collection initiatives directed by CDC to monitor sudden unexpected infant deaths, reduce infant mortality and build epidemiological support at the state and local level to improve maternal and child health programs.
A variety of efforts are underway to increase workforce diversity and expand access to doula and other services to improve maternal and infant health outcomes and reduce disparities. Studies have shown that a more diverse healthcare workforce and the use of doulas may improve birth outcomes. The percent of maternal health physicians and registered nurses that are Hispanic or Black is lower than their share of the female population of childbearing age. The Biden Administration’s Blueprint includes efforts by HRSA to develop a maternal care pipeline to provide scholarships to students from underrepresented communities in health professions and nursing schools to grow and diversify the maternal care workforce. The use of doula services is another approach to increase diversity and expand the maternal health workforce. Doulas are trained non-clinicians who assist a pregnant person before, during and/or after childbirth by providing physical assistance, labor coaching, emotional support, and postpartum care. Pregnant women who receive doula support have been found to have shorter labors and lower C-sections rates, fewer birth complications, are more likely to initiate breastfeeding, and their infants are less likely to have low birth weights. The Biden Administration’s Blueprint includes a FY2023 budget request for $20 million to grow and diversify the doula workforce. Additionally, in recent years there has been growing interest in expanding coverage of doula services through Medicaid . Federal legislation has been introduced to expand coverage of doula services through Medicaid, and some states are taking steps to include coverage through their state programs. State efforts to date have had mixed success, in part because of challenges with certification requirements and low reimbursement levels. In 2022, there were at least 17 states considering, planning, or implementing coverage of doula services through Medicaid reimbursements. Some states are also implementing or expanding coverage for other services focused on improving maternal and infant health including home visiting programs to teach positive parenting and other skills; postpartum services provided by lactation counselor and consultants, public health nurses, and medical caseworkers; as well as targeted case management and other programs to meet needs of pregnant and postpartum individuals with substance use disorders.
States, providers and health systems, foundations, and communities also are engaged in a broad range of efforts to advance maternal and child health and reduce disparities. Several states have developed plans and initiatives to address disparities in maternal and infant outcomes. For example, New Jersey launched the Nurture NJ Strategic Plan to outline challenges, action areas, and recommendation to achieve equity for all women with a focus on dismantling structural racism and addressing social determinants of health. In addition, many state Medicaid programs have implemented policies, programs, and initiatives to improve maternity care and outcomes and , including expanding eligibility for people during and after pregnancy, conducting outreach and education to enrollees and providers, expanding coverage for benefits such as doula care, home visits, and substance use disorder and mental health treatment, and using new payment, delivery, and performance measurement approaches. Also, five states reported including Performance Improvement Projects (PIPS) for their Medicaid services that focused specifically on reducing disparities related to maternal and child health in Fiscal Year 2022, including Illinois, Michigan, Minnesota, Nevada, and Texas. California is in the process of implementing provisions from legislation passed in recent years requiring implicit bias training for all perinatal health workers, as well as elements of the California MOMNIBUS , which directs the state to invest in improved data analysis, streamlining administrative procedures within the welfare program for pregnant people, and broadening the midwifery workforce. Northwell Health , the largest healthcare provider in New York, recently launched a Center for Maternal Health to address pregnancy related health risks facing Black women by seeking to address issues within healthcare and in the community that arise before, during, and after pregnancy. The Changing Woman Initiative is a Native American midwifery organization in New Mexico providing culturally centered care to address maternal health disparities, high rates of gestational diabetes, and low birth weight deliveries among Indigenous women.
A range of organizations are advocating for more interventions and supports to address maternal mental health and substance use issues, major causes of pregnancy-related mortality and morbidity. The field of maternal mental health and substance use encompasses a large range of conditions that affect the health of parents and their infants. Some studies have found higher rates of postpartum depression among some pregnant and postpartum women of color, but many mental health conditions are undiagnosed and untreated due to stigma and poor access to treatment. These issues also limit access to services for pregnant and postpartum people suffering from substance use disorders. Community-based and provider organizations are calling for a number of policy and structural changes to address these large challenges, including broader insurance coverage for behavioral health care, higher reimbursement for existing treatment services, greater education and awareness about screening for mental health and substance use conditions among health care providers and childbearing people. Federal initiatives in this area include CMS’ Maternal Opioid Misuse (MOM) Model , a grant program for states to better integrate care for mothers and infants exposed to opioids, and state-level learning communities on mental health, supported by the Health Resources and Services Administration (HRSA) .
At the same time many efforts are focused on improving maternal and infant health and reducing disparities, the recent overturning of Roe v. Wade may contribute to widening disparitie s in maternal and infant health , People of color are likely to be disproportionately affected by state actions to fully prohibit or implement extensive restrictions on abortions as they are more likely to seek abortions and more likely to face structural barriers that will make it more difficult to travel out of state for an abortion, including more limited access to health care and fewer financial and transportation resources. Increased barriers to abortion for people of color may widen the already existing large disparities in maternal and infant health, have negative economic consequences for families, and increase risk of criminalization for pregnant people of color.
Looking Ahead
Overall, these data show that racial disparities in maternal and infant health persist. Improving maternal and infant health is key for preventing unnecessary illness and death and advancing overall population health. Healthy People 2030 , which provides 10-year national health objectives, identifies the prevention of pregnancy complications and maternal deaths and improvement of women’s health before, during, and after pregnancy as a public health goal. The COVID-19 pandemic further highlights the urgency and importance of addressing disparities in health more broadly and increased attention to disparities in maternal and infant health specifically. Moreover, the overturning of Roe v. Wade may contribute to worsening disparities in maternal and infant health, further amplifying the importance of attention to these areas.
The increased awareness and attention to maternal and infant health have contributed to a rise in efforts and resources focused on improving health outcomes in these areas and reducing disparities. These include efforts to expand access to coverage and care, increase access to a broader array of services and providers that support maternal and infant health, diversity the health care workforce, and enhance data collection and reporting. However, addressing social and economic factors that contribute to poorer health outcomes and disparities will also be important. Moreover, the persistence of disparities in maternal health across income and education levels, points to the importance of addressing the roles of racism and discrimination within and beyond the health care system as part of efforts to improve health and advance equity.
Data and research often assume cisgender identities and may not systematically account for people who are transgender and non-binary. The language used in this brief attempts to be as inclusive as possible while acknowledging that the data we are citing uses gender labels that we cannot change without misrepresenting the data.
← Return to text
- Racial Equity and Health Policy
- Women's Health Policy
- Race/Ethnicity
- Maternal and Child Health
news release
- Updated Brief on Racial Disparities in Maternal and Infant Health
Also of Interest
- Medicaid Postpartum Coverage Extension Tracker
- How Does the ACA Expansion Affect Medicaid Coverage Before and During Pregnancy?
Health Care Access and Quality
Goal: increase access to comprehensive, high-quality health care services..

Many people in the United States don’t get the health care services they need. Healthy People 2030 focuses on improving health by helping people get timely, high-quality health care services.
About 1 in 10 people in the United States don’t have health insurance. 1 People without insurance are less likely to have a primary care provider, and they may not be able to afford the health care services and medications they need. Strategies to increase insurance coverage rates are critical for making sure more people get important health care services, like preventive care and treatment for chronic illnesses.
Sometimes people don’t get recommended health care services, like cancer screenings, because they don’t have a primary care provider. Other times, it’s because they live too far away from health care providers who offer them. Interventions to increase access to health care professionals and improve communication — in person or remotely — can help more people get the care they need.
Objective Status
Learn more about objective types
Related Objectives
The following is a sample of objectives related to this topic. Some objectives may include population data.
Health Care Access and Quality — General
- Adolescents
Drug and Alcohol Use
Family planning.
- Health Care
Health Communication
- Health Insurance
- Oral Conditions
Pregnancy and Childbirth
Sensory or communication disorders, sexually transmitted infections, other topics you may be interested in.
Berchick, E.R., Hood, E., & Barnett, J.C. (2018). Health Insurance Coverage in the United States: 2017. Retrieved from https://www.census.gov/content/dam/Census/library/publications/2018/demo/p60-264.pdf [PDF - 1.4 MB]
The Office of Disease Prevention and Health Promotion (ODPHP) cannot attest to the accuracy of a non-federal website.
Linking to a non-federal website does not constitute an endorsement by ODPHP or any of its employees of the sponsors or the information and products presented on the website.
You will be subject to the destination website's privacy policy when you follow the link.
- Open access
- Published: 29 April 2024
A qualitative study of the barriers to commissioning social and therapeutic horticulture in mental health care
- Carly J. Wood 1 ,
- Georgina Morton 1 ,
- Kathryn Rossiter 2 ,
- Becs Baumber 2 &
- Rachel E. Bragg 1 , 3
BMC Public Health volume 24 , Article number: 1197 ( 2024 ) Cite this article
688 Accesses
6 Altmetric
Metrics details
Social and Therapeutic Horticulture (STH) is a process where trained practitioners work with plants and people to improve an individual’s physical and psychological health, communication and thinking skills. Evidence suggests that STH can support individuals with mental ill-health, however, current commissioning of STH within mental health care is limited. This study aimed to understand the barriers to commissioning STH in mental health care and to identify potential solutions to barriers, to support more widespread availability of services.
Individuals with a role in mental health care commissioning from across the UK were invited to take part in semi-structured interviews via zoom. Interviews explored factors influencing the mental health services they commission or refer to, their perception of the role of STH in mental health care and the barriers to commissioning STH, together with potential solutions to any barriers identified.
Commissioners identified a lack of knowledge of STH and evidence of its effectiveness, and a culture which prioritises traditional medical models, as barriers to commissioning. Challenges for STH providers in responding to large-scale commissioning requirements were also highlighted as a barrier.
Conclusions
To upscale commissioning of STH in mental health care, STH interventions need to be embedded within NHS priorities and information on STH services and their effectiveness needs to be easily accessible to practitioners. The sector should also be supported in working collaboratively to enable commissioning of services at scale.
Peer Review reports
Mental health is defined as “a state of well-being in which every individual realises their own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community” [ 1 ]. Mental illness or mental ill-health is characterized by a clinically significant disturbance in an individual’s cognition, emotional regulation, or behaviour, that is associated with distress or impairment in important areas of functioning, such as work, daily activities, or personal relationships [ 2 ]. The NHS identify five mental health levels which capture both mental health and mental illness on a continuum [ 3 ], moving from Level 0, where a person can take their own decision to independently improve their mental health and wellbeing, through to level 4, a person who is experiencing acute mental health crisis or who has a long-term serious mental illness. It is expected that people move through the different mental health levels either on a recovery pathway, or during times when mental health worsens and an increased level of intervention is required.
Common treatment approaches for mental health levels 2 and above include medication and psychological therapies [ 4 ]. However, medications such as anti-depressants may only provide significant positive effects for severe depression (level 4) [ 5 ] and have side effects or withdrawal symptoms [ 6 ]. Recent clinical trials also indicate that the efficacy of psychological therapies such as cognitive behavioral therapy (CBT) has diminished [ 7 ] whilst long waiting lists [ 4 ], can leave individuals without treatment for significant periods of time.
Social and Therapeutic Horticulture (STH), a process where trained practitioners work with plants and people to improve an individual’s physical and psychological health, communication and thinking skills [ 8 ], is one type of nature-based intervention (NBI) that is used to support individuals with mental ill-health. Although often used as an umbrella term for all gardening activities that target health and wellbeing, STH represents more targeted gardening activities that support individuals at mental health levels 2 and 3, typically provided by the voluntary, community and social enterprise (VCSE) sector. More specialised provision (termed ‘horticultural therapy’) for level 4 mental health needs where patients are typically in hospital or in-patient settings, and less specialised social gardening for level 1 needs is also available.
To date, multiple systematic reviews and meta-analyses have been conducted on the benefits of gardening and STH activities, reporting reductions in symptoms of depression and anxiety, reduced stress and mood disturbances, and improved quality of life, life satisfaction and community belonging for a range of groups, including the general public, patients with a range of physical illnesses, those with poor mental health, symptoms or diagnoses of mental illness [ 9 , 10 , 11 , 12 , 13 , 14 , 15 ]. In a recent review of randomised controlled trials (RCTs), Briggs, Morris, and Rees [ 16 ] revealed an overall positive effect of STH interventions for depression and wellbeing, with half of the included studies involving individuals with a diagnosis or symptoms of mental illness. Despite the positive findings from this review, much of the existing evidence of the benefits of STH is focused on gardening and gardening activities for individuals at mental health level 0 and 1. There are fewer published scientific studies specifically focusing on individuals at mental health levels 2–4 who would need to be referred to STH interventions. Furthermore, most published studies use pre-post design methodologies without control groups, and incorporate a variety of outcome measures, thus making it difficult to combine findings across studies.
Despite evidence of the benefits of STH for a range of populations, and an increased interest from the Government and NHS [ 17 ] in the health and wellbeing benefits of engaging with nature, referrals to STH are not widespread from the NHS or within social prescribing schemes [ 18 ]. Current commissioning of NBI such as STH are primarily from the local authority, social services, self-referrals, special education, and Community Mental Health Teams [ 18 , 19 ], rather than routinely from general practitioners (GPs) or other clinicians. The NHS commissioning cycle involves a continual process of (i) strategic planning (to identify needs, review provisions and decide priorities); (ii) procurement of services and (iii) monitoring and evaluation [ 20 ]. Given that the NBIs have been highlighted as a key priority for improving mental health [ 17 ], wider commissioning might be expected. However, Shaw et al. [ 21 ] highlighted that commissioning for long term conditions is labour intensive for commissioners, with the scale and intensity of the work often not being proportionate to the service gains. It was also reported that commissioners were less comfortable with the transactional elements of their role, such as decommissioning services or seeking new providers [ 21 ]. These factors might act as barriers to commissioning of STH for mental health.
There has recently been a fundamental shift in the way that the health and care system is organized in the UK. In July 2022, Integrated Care Systems (ICS) were given statutory status, with Integrated Care Boards (ICBs) being set up to take on the NHS planning functions previously held by clinical commissioning groups, enabling joined up working and partnerships between health and social care and VCSE organisations [ 22 , 23 ]. It was hoped that this shift might result in increased commissioning of services based in VCSE sector, however, there also may be unique and unknown challenges experienced within this new structure. The aims of this study were therefore to (i) understand the barriers to commissioning STH in mental health care and (ii) identify potential solutions to these barriers to support more widespread availability of services.
To understand barriers to commissioning STH in mental health care, a combined deductive and inductive qualitative approach was used [ 24 ]. Semi-structured interviews, a common qualitative method, were conducted to obtain in-depth information about the experiences and perspectives of individuals with a role in mental health care commissioning. The interviews were conducted by a research assistant trained in qualitative data collection techniques and analysis.
Study context
Potential participants were identified by the research team and members of the Therapeutic Horticulture Stakeholder Group (THSG), a group established by Natural England in March 2022 with support from The National Academy of Social Prescribing (NASP), to explore how to grow the Therapeutic Horticulture offer and to support the scaling up of Green Social Prescribing (GSP) [ 25 ]. The group (currently chaired and convened by Thrive with support from Natural England) brings together leading organisations and professionals in this field with representation from Natural England, The National Academy of Social Prescribing (NASP), NHS England, academics, health care professionals, and organisations who support the provision of STH. With permission, THSG members provided the research team with the email addresses for individuals with a role in mental health care commissioning who might be interested in taking part in the research.
Recruitment
Individuals were purposively selected for participation in the research based on their job role to ensure representation across mental health ‘commissioning’ roles, including individuals who refer individual patients to mental health services through to those in senior positions with responsibility for commissioning regional mental health services. Participants were also selected to incorporate the perspectives of individuals both with and without experience of commissioning or referring to STH interventions and from across multiple regions of the UK. All potential participants were contacted via email by a member of the research team and provided with information about the study via a participant information sheet. Potential participants also shared information about the research with their colleagues who were also invited to take part in the study. A combined purposive and snowballing sampling approach was therefore used, two sampling techniques that are commonly combined [ 26 ]. In total 22 participants were invited to participate in the study.
Prior to participation in the research, participants were sent the definition of STH [ 8 ] and the mental health levels [ 3 ] to aid discussion of the role of STH in mental health care and to ensure consistency in their understanding of both STH and the NHS mental health levels. All participants provided informed consent prior to participation in the study and reconfirmed their consent at the start of the interview. Ethical approval was granted by Ethics Sub-committee 2 at the University of Essex (ETH2223-0519). Regulations regarding data management and storage were adhered to throughout the research.
Characteristics of participants
Nine participants provided consent to take part in an online semi-structured interview via zoom, including five males and four females. Participants were from a range of roles related to mental health care, with some participants referring individual service users to local services and others commissioning services for an entire region. Participants were a link worker, a GP, a consultant psychiatrist, a clinical psychologist, a commissioner of mental health services for children and young people, a community mental health team project manager, director of adult mental health, head of commissioning and policy, and a mental health programme lead. Most participants ( n = 5) reported having a general awareness of GSP and NBI but no expertise in STH, whilst the remaining participants ( n = 4) reported extensively researching STH and commissioning or supporting STH-type services. Participants were from multiple regions across the UK (with two participants spanning two regions), including Essex ( n = 4), Suffolk ( n = 1), Lancashire ( n = 1), South Cumbria ( n = 2), Somerset ( n = 1), Kent ( n = 1) and Manchester ( n = 1).
Semi-structured interviews were conducted between February-April 2023. Interviews were conducted electronically in a private space at the participants and researcher’s place of work or in their homes. Interviews lasted between 17 min and 47 min, with this variation in duration resulting from the mixed experiences of STH amongst participants. Interviews were recorded using Zoom software and automated transcripts downloaded, checked, and corrected by the research assistant prior to analysis. All participants were asked about their job role, the factors that influence the mental health services they commission or refer to, their perception of the role of STH and the barriers to commissioning STH, together with potential solutions to any barriers identified. The topic guide used in the interviews is included in Appendix 1 . This guide was developed by the authors, in line with the study aims, with feedback provided by the THSG to refine the final interview guide.
Data were managed and coded using NVivo software version 12 (QSR International Pty Ltd., Doncaster, Australia, 2018). Transcripts were coded using reflexive thematic analysis, following the phases of Braun and Clarke [ 27 , 28 ]. Initially, two interview transcripts were coded independently by two authors (CJW, GM) and following discussion, a coding framework was developed and used to code the remaining transcripts. The coding framework was revised as coding continued. Themes were actively produced through exploration of the data and codes, and subsequent discussions between the wider research team.
As data analysis progressed and themes developed, the researchers discussed their own assumptions of the codes and themes. The researcher with the least experience in the mental health benefits of STH carried out the primary analysis to ensure that there was the least bias in the coding of the data. In the final stage of the analysis, four overarching themes were identified, each of which are described in detail below and include funding and workforce (theme 1), commissioning culture (theme 2), knowledge of STH (theme 3) and evidence of effectiveness (theme 4). Within these themes both the barriers to commissioning STH in mental health care (aim 1) and potential solutions to the barriers raised (aim 2) are discussed.
Theme one: funding and workforce
A lack of funding available for mental healthcare in the NHS was referred to as a key challenge for commissioning by most participants. Participants referred to a reduction in investment in mental health services over the last decade and reflected that a consequence of the reduced investment was that the NHS was “ trying to do more with less ”. Commissioning decisions were therefore suggested as being based around what can be delivered given the finances available and ensuring that commissioned services are “ cost effective ”. Commissioners were reported as being left in a position where they must commission based on what they can afford to provide rather than based on what they perceive to be best for their population.
In relation to STH specifically, most participants reported that the limited budgets available for mental health care result in sustainable and longer-term funding being a persistent problem for VCSE organisations. This was thought to result in the short-lived nature of STH services and high staff turnover. The lack of consistency in the offer across regions was also thought to compound this problem. Participants commented on the need to commission services that can cater for the entire population for which they commission, with “ pockets of services” making it difficult to do so. These “ pockets of services ” were deemed as not always being in areas where they were most needed, being less cost-effective, not being accessible for all and potentially requiring transportation to reach, which may pose financial issues for both individuals and organisations.
“They don’t want to be having just one project in one corner of their patch. They want to be able to say we’re doing this across the whole county.” (General Practitioner)
It was suggested that partnership working within the VCSE sector would enable a more consistent offer and a larger “ footprint” across regions, which would support access to larger funding streams, the growth of smaller VCSE organisations and subsequently wider scale commissioning of services.
Similar to a shortage of funding, most participants referred to a lack of workforce and resources within mental health services. One participant referred to a “revolving door of personnel” , resulting in continued staff shortages, whilst another referred to the constant juggling of resources. These issues were suggested to be a barrier to commissioning of new services such as STH.
“...new idea is...something they've not got time for as they’re so bogged down, it’s just kind of surviving day to day really. It’s almost too much to start thinking about something new, like a new nature-based therapy group.” (Clinical Psychologist)
One participant reported that the loss (and lack of replacement) of staff in particular roles essential to furthering the NHS Trusts green plans and working with the VCSE sector, further limited commissioning of STH. It was felt that embedding sustainability roles into Trusts would save money and that having directors and ‘champions’ who have a personal interest in sustainability, would help to influence commissioning boards and push the sustainability and STH agenda forward. However, the association between sustainability roles and commissioning of STH was only made by one participant, making it unclear to what extent these are reliant upon each other.
It was also reflected by one participant that the underfunding and understaffing issues within the NHS might present a key opportunity for the VCSE sector to assist in providing mental health care if it is given the chance, with another participant referring to the “missed opportunity” within their Trust to use small pots of funding to support the VCSE sector.
Theme two: commissioning culture
Several participants suggested that commissioned mental health services are driven by national requirements set out by the NHS and in the long-term plan [ 29 ] and that services such as STH are “not really embedded in national must dos…” Rather than facilitating a holistic approach to commissioning, the NHS guidelines (combined with the underfunding and under-resourcing of mental health care) were thought to limit the capacity of commissioners to allocate funding for services within the VCSE sector. Participants emphasised the need to see “ green initiatives ”, “ efforts ” and “ schemes ” within these national plans to support the commissioning of STH.
The commissioning culture of a “focus on reactive treatments rather than prevention” , was also reflected as a barrier to commissioning STH, with several participants discussing prevention of mental illness in relation to STH. Traditional approaches and therapies (i.e., talking/cognitive and drug therapies) were suggested as being prioritised, with a need to shift towards more preventative and holistic treatment in order for services like STH to be fully embedded.
“I think what we’re trying to do is stop the knee-jerk reaction to ‘we have to plug a gap over here’ and thinking about it more creatively and that’s what we’re trying to do. But it’s a big shift for the system, and it’s really easy to just keep throwing money at something that is a traditional approach to fixing something”. (Commissioner of mental health services for Children and Young People)
Some participants also suggested that STH should be embedded at every level of mental health care, allowing patients at all levels of mental health need to be referred to VCSE sector services and via a number of different referral pathways.
“It’s obvious, you build it in at all levels of referral...before GP, at GP, at IAPT [Increasing Access to Psychological Therapies], at secondary care. You just open the doors, and it would be successful. Reduce the demand on the NHS” (Consultant Psychiatrist).
It was felt that this approach would support individuals in accessing STH services, but that in order for it to be embedded at every level there would need to be “buy-in” from commissioners.
Theme three: knowledge of STH
Whilst all participants felt that there was a role for STH in mental health care, a lack of knowledge of STH by individuals with roles in referrals and commissioning was reported as a barrier to commissioning. While some participants within the study demonstrated or reported good knowledge of what STH is, the services available, and the range of mental and physical health benefits it could provide, this was cited as not being the case for all individuals within their organisations, where there was a mixture of different levels of knowledge. Some study participants also reported (or demonstrated) that they personally had limited knowledge of what STH is, who it is for and/or the evidence base surrounding the health benefits. There were some perceptions that STH would only appeal to certain groups and that it could only play a role in mental ill-health prevention or maintenance rather than in treatment, which contradicts the evidence supporting the use of STH in health care.
“This type of activity probably appeals to people in a particular demographic...I'm not necessarily convinced that people in their twenties and thirties would think of that as a go-to for leisure, pleasure, or seeing that as something that would benefit them..”. (Head of Commissioning and Policy)
The limited knowledge of STH was largely attributed to a lack of available information from providers of STH about the benefits of their services, who they are targeting, and how risk is managed. Most participants reported not receiving information or it not being readily available or easily accessible amongst the large volume of information that commissioners already receive. Some participants also referenced the need for the VCSE sector to promote or ‘champion’ their services and directly approach the NHS to highlight what they were doing within the community and to identify how this might align with ongoing NHS agendas.
“We need to be able to understand what the offer is, and it’s not always clear what community assets are available, and so I think the sector could do a better job for sure of collating those offers. But we need to understand what it is, what the needs are, what the value is, and how we can support it in a financially challenged environment.” (Community Mental Health Team Project Manager)
Overall, participants felt that greater and more effective sharing of information on STH and communication with commissioners was needed for STH to be commissioned more widely.
“Why are we not doing it? We don’t really know what they’re doing”. (Link Worker)
This was felt to be particularly important given that commissioners do not typically get training in STH.
Theme four: evidence of effectiveness
Evidence was highlighted as a factor influencing commissioning by all participants involved in the study, but to varying degrees and in varying contexts, perhaps reflecting differences in the knowledge of participants. Evidence of the effectiveness of STH was perceived by several participants as lacking in quantity and quality, with some reference to the need for high quality studies. Some participants also referred to a lack of awareness of evidence of the benefits of STH, in line with a lack of knowledge of STH broadly (Theme 3). However, one participant with extensive experience of STH, said that lack of evidence in relation to the benefits of STH was not the issue but rather a lack of evidence of how STH can “ structurally work within government commissioned services ”, alluding to potential difficulties in embedding services such as STH throughout the healthcare system.
Some participants also referred to the differences in evidence between levels of mental health need and how it was not necessarily effective for all mental health conditions, with one participant stating that it is not a “universal panacea” . One participant referred to the evidence of STH for severe and enduring mental illness and that whilst there was evidence to support its use, it was not widely publicised. Participants felt that evidence of the benefits of STH needed to be shared widely, easy to access and regularly updated.
“..the longer you work as a doctor, the less you become an academic because you become a clinician, so it’s less easy to access all that information. So, it’s a bit difficult to kind of prove to people that there is some decent evidence.” (Consultant Psychiatrist)
Several participants also referred to key performance indicators that the NHS are measured against and the need for STH services to have measurable outcomes that align with these indicators, for example the Warwick Edinburgh Mental Wellbeing Scale. A number of participants also commented that these outcomes should be focused on the effect STH has had on the individual patient, instead of statistics like waiting, access and discharge rates, which do not identify whether the patients’ condition has improved. However, there were also contradictory points highlighting that commissioning decisions were typically based around referral and discharge rates, the longer-term impacts on the healthcare system, and cost savings for the NHS, with these statistics being easier to examine than the impacts on patients.
As a result of challenges over measurement of outcomes and impact, some participants suggested changes to the ways that STH providers collect and provide evidence. Participants recommended that the sector focuses on providing qualitative evidence such as “ case studies ”, “ vignettes ” or “ user experience voices ” that tell “ the positive story ” of the impact their service has for the individual.
“...Health has a high bar for reporting, and we need to be able to prove that something has had an impact.. We can’t do the same thing really, with some of the green investments that we make. And so, I think we need to understand how we can evidence the impact it’s had, and it doesn’t always need to be data driven ...There are number-driven discussions, or data driven discussions. What is missing in that room is the patient’s story and the impact. And I think that’s where the third sector could really help us bring this to life.” (Community Mental Health Team Project Manager)
However, this type of evidence was acknowledged as being difficult to accomplish and often limited by the infrastructure of the organisations who may not have the capacity to collect this information. One participant suggested that if this evidence was available, the use of a video to demonstrate the impact on patients might be a technique that would “sell” the service to commissioners.
The aims of this study were to (i) understand the barriers to commissioning STH in mental health care and (ii) identify potential solutions to these barriers to support more widespread commissioning of STH services. The key themes that were produced from the data were issues around funding and workforce which prevented widespread commissioning of STH, a commissioning culture which makes it difficult to commission ‘non-traditional’ treatments, a lack of knowledge of what STH is and how it can be used, the services available, and a lack of [awareness of] evidence to support its effectiveness. There were a number of suggestions as to how these barriers could be overcome, most of which are likely to require systems-level change by both the NHS and VCSE sector.
In relation to funding and workforce, the continued reductions in funding for mental health care were identified as a key barrier to commissioning STH. This finding is mirrored in the recent evaluation of the Government’s GSP pilot, which identified unstable short-term funding and lack of system level support for the sector as a barrier to embedding GSP within statutory systems [ 22 ]. Furthermore, the recently established, ICBs, which were designed to support greater partnership working with the VCSE sector, have been asked to make a further 30% reduction in their running costs [ 30 ]. As a result, funding and resources for mental health services are likely to become even more stretched, further restricting commissioning of new services.
In the UK most NBIs, including STH, sit within the VCSE sector and are typically delivered by small-scale providers, allowing for a more bespoke, person-centred service [ 22 , 31 ]. However, this approach makes it difficult for STH providers to respond to large-scale commissioning requirements and combined with the funding and resources issue, is likely to result in commissioners continuing to consider STH as a less viable option for mental health care. Thus, it is essential that STH providers work in partnership to demonstrate the ‘offer’ for services they can provide on a regional scale [ 32 , 33 ]. This collaborative approach could be supported and facilitated through the use of regional nature-based VCSE networks such as the Norfolk Green Care Network [ 34 ] and the Reading Green Wellbeing Network [ 35 ]. These networks can promote partnership working between providers, become potential commissioning hubs and could enable providers to work together to apply for larger funding opportunities. Voluntary networks such as these could also help ICBs proactively engage with VCSEs but would need investment and support at the system-wide level to ensure sustainability.
Commissioning culture within the health service was also identified as a key barrier to commissioning of STH. Despite a commitment to increase use of personalised care, social prescribing, and community centred approaches for health and wellbeing across multiple Government and health organisations [ 36 , 37 ], the NHS long plan [ 29 ], which outlines the key priorities from 2019 to 2024, does not embed the use of these approaches as priorities. Instead, it prioritises helping people to get easier access to therapy for common mental disorders such as anxiety and depression; despite evidence to suggest diminishing effectiveness over time and poor outcomes for some groups [ 7 ]. Without community-based approaches being embedded within national plans, participants felt they had limited capacity to commission the VCSE sector.
The recently published NHS major conditions strategy case for change and strategic framework [ 38 ] calls for a focus on integrated working with community-based partners as part of the future long term conditions strategy, and a commitment to accelerating research to understand how mental, physical, and social conditions interlink and how they can be treated. Given that services such as STH can target mental, physical, and social needs simultaneously [ 39 ], it is possible that this focus may result in increased use of holistic services such as STH. However, until the full long-term conditions strategy is released, it is unclear how these approaches will be embedded and prioritised. As highlighted by participants, for interventions such as STH to be successful, they need to be embedded at every level of mental health care, allowing multiple entry points into the VCSE sector. The trend for prioritisation of traditional approaches to mental health care, as also reported by Shanahan et al. [ 40 ] and Tambayah et al. [ 41 ], alongside the suggested reluctance of commissioners in decommissioning services and seeking new providers [ 21 ], also needs to be overcome to promote greater variability in treatment options.
Lack of knowledge and awareness of STH, in a variety of contexts, was highlighted as a key barrier to service commissioning. There were some perceptions that STH would not appeal to all individuals or that it was not suitable for particular groups, for example younger people. A lack of knowledge about what STH interventions entail and the level of mental health need they can be appropriate for, was also highlighted by participants, with some interviewees referring to STH as solely a preventative health measure as opposed to a treatment option for acute and chronic mental illness. Furthermore, a lack of knowledge and awareness of what STH provision is available was identified as a barrier to commissioning. Lack of knowledge of local services has also been identified as a barrier to commissioning NBIs via GSP [ 22 ] and for commissioning STH by clinicians [ 42 ]. As commissioning of new services requires significant partnership working between both commissioners and service providers [ 21 ], this lack of awareness of what STH services are available locally is likely to be problematic.
Shanahan et al. [ 40 ] and Fixsen and Barrett [ 43 ] highlighted that referral and commissioning of NBI is influenced by the knowledge and interest of the GP, termed “GP buy-in” . Thus, individuals may not be offered interventions such as STH unless their health care provider has a particular interest in, knowledge of, or belief in its value. This need for ‘practitioner buy-in ’ is not aligned with traditional approaches where treatments are prescribed as ‘normal practice’ regardless of whether the practitioner has a particular interest in the approach. Providing a means by which practitioners can easily access information about STH services, such as regional or national directories of STH services, which enable identification of interventions across the UK and detail what they involve and who they are for, may facilitate increased awareness, knowledge and ‘ buy- in’ of STH interventions. However, any directory would need to be fully embedded in healthcare treatment, referral, and commissioning systems.
An interesting observation that emerged from the data was also the tendency of participants to refer to STH as green “schemes” , “therapies” or “initiatives” , indicating a perception that all nature-based activities are equivalent as reported by Sempik, Hine and Wilcox [ 44 ]. This is problematic and is likely to compound issues around what types of STH services are appropriate for different levels of need. To address this barrier, a framework for aligning STH provision with the NHS’ five mental health levels has been produced, identifying what types of activities, support, evaluation, and quality assurance are needed at each level, along with examples of beneficiaries across the UK [ 45 ]. To support partnership working, increased understanding and commissioning of STH, this framework should be adopted widely by both the health care sector and STH organisations and utilised in the suggested service directory.
Evidence of the effectiveness of STH was mentioned by all study participants as a factor that influences commissioning. Whilst some referred to a lack of awareness and publicisation of the evidence, as echoed in Tambayah et al. [ 41 ], others reported a lack in quality and quantity, or a lack of evidence for specific mental health levels or conditions. For individuals at mental health levels 0 and 1, there are a range of systematic reviews and meta-analyses demonstrating the benefits of gardening activities [ 11 , 12 , 14 , 15 ]. There are also numerous studies and reviews reporting the benefits for STH for individuals with symptoms of mental illness or diagnosed mental illness, aligning with mental health levels 2–4. However, in many cases this data is combined with data from individuals without mental ill-health, or for a range of mental health disorders [ 13 , 16 , 46 ], making it more difficult to isolate the evidence for specific conditions and those who require mental health intervention. Whilst studies focused on individuals at levels 2–4 with mild to severe mental illness have demonstrated positive effects for depression, wellbeing, quality of life and activities of daily living [ 16 , 47 ], many studies fail to incorporate comparison groups or randomisation procedures. To further enhance the evidence base, well-designed, high quality RCTs are therefore needed, along with sufficient funding to support this level of scientific evaluation.
Whilst there is undoubtedly room for high quality RCTs to further advance the STH evidence base, other accepted interventions in health and policy fields in the UK have not been based on RCT evidence [ 48 ]. There is also a wealth of quantitative and qualitative evidence from the scientific and VCSE sector advocating the effectiveness of STH, much of which utilises measurable outcomes and describes the impact on the patient (as suggested by the study participants). Furthermore, an independent report by the Kings Fund [ 48 ] suggested that gardening-based interventions can have numerous benefits for individuals as an adjunct to their existing mental health treatment, whilst the Wildlife Trusts [ 49 ] demonstrated significant cost savings to the NHS if they were to invest in a ‘natural’ health service, with an estimated an annual cost of £534.1 million per year for delivery against a gross annual cost saving of £635.6 million. Thus, whilst there is need to strengthen the evidence base in specific areas, there is clear evidence of the potential benefit of NBIs such as STH to the health care system and patients. Furthermore, Wye et al. [ 50 ] reported that commissioners experience multiple barriers to using academic research to inform commissioning. As a result, they often utilise NICE guidelines, local evaluations, local clinicians’ knowledge, and service users experiences to inform their commissioning decisions. To support commissioning of STH, existing evidence and knowledge should be integrated into mental health care policy and practice, NICE guidelines, and be more clearly publicised and communicated to commissioners via effective dissemination methods such as infographics and via professional journals aimed at commissioners.
The findings of this study present the perspectives of nine individuals, from a range of commissioning roles and regions across the UK. However, the full range of barriers experienced by individuals with roles in mental health care commissioning may not have been captured. Further research in this field should aim to incorporate the perspectives of individuals involved in the development of mental health policy and NHS senior leaders who have a direct influence on funding decisions, to understand the barriers to prioritising approaches such as STH at a national level. It should also prioritise high quality RCTs for mental health levels 2–4 and for specific conditions, to develop a clearer and more focused evidence base to support commissioning of STH in mental healthcare. The potential solutions to the commissioning barriers highlighted in this research should also be actioned by individuals in health and VCSE sectors to further support the growth and commissioning of STH. This is essential for ensuring a more sustainable mental health system whereby service users can access support when it is needed.
Overall, the findings of this study highlight a range of barriers to the commissioning of STH, including a commissioning culture which priorities traditional medical models, a lack of knowledge of STH broadly (including the services available, levels of mental health need it can cater for and the existing evidence of its effectiveness, particularly for specific mental health conditions), and the challenges for STH providers in responding to large-scale commissioning requirements. To support commissioning of STH in mental health care, the VCSE sector should be supported in developing higher quality evaluation methodology accepted by the NHS and in working collaboratively to enable commissioning of services at scale. Information on STH services and their effectiveness also needs to be easily accessible to practitioners, and STH interventions should be fully embedded within NHS priorities to enable a more holistic health care approach, which has the potential to improve patient outcomes, reduce the strain on mental health services and result in considerable cost savings.
Availability of data and materials
The datasets generated during the current study are available in the REShare repository, with restricted access via https://reshare.ukdataservice.ac.uk/856812/ .
Abbreviations
Cognitive Behavioural Therapy
General Practitioner
Green Social Prescribing
Integrated Care Board
Integrated Care System
Nature-based Intervention
National Health Service
Randomised Controlled Trial
Social and Therapeutic Horticulture
Voluntary, Community and Social Enterprise
World Health Organisation. Mental Health: Strengthening Our Response. 2022. https://www.who.int/news-room/factsheets/detail/mental-health-strengthening-our-response . Accessed 8 Aug 2023.
World Health Organisation. Mental Disorders 2022. 2022. https://www.who.int/news-room/fact-sheets/detail/mental-disorders . Accessed 8 Aug 2023.
NHS England. Green Social Prescribing Toolkit, London UK, England NHS. 2023. https://socialprescribingacademy.org.uk/media/3ozd3tv2/nhs-green-social-prescribing-toolkit.pdf . Accessed 8 Aug 2023.
Aughterson H, Baxter L, Fancourt D. Social prescribing for individuals with mental health problems: a qualitative study of barriers and enablers experienced by general practitioners. BMC Fam Pract. 2020;21:194. https://doi.org/10.1186/s12875-020-01264-0 .
Article PubMed PubMed Central Google Scholar
Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam JD, Shelton RC, Fawcett J. Antidepressant drug effects and depression severity: a patient-level meta-analysis. JAMA. 2010;303:47–53. https://doi.org/10.1001/jama.2009.1943 .
Article CAS PubMed PubMed Central Google Scholar
Taylor S, Annand F, Burkinshaw P, Greaves F et al. 2019. Dependence and Withdrawal Associated with Some Prescribed Medicines: An Evidence Review. London, UK: Public Health England, 2019. https://assets.publishing.service.gov.uk/media/5fc658398fa8f5474c800149/PHE_PMR_report_Dec2020.pdf . Accessed 9 Aug 2023.
Johnsen TJ, Friborg O. The effects of cognitive behavioral therapy as an anti-depressive treatment is falling: a meta-analysis. Psychol Bull. 2015;141:747–68. https://doi.org/10.1037/bul0000015 .
Article PubMed Google Scholar
Thrive. Social and Therapeutic Horticulture. 2023. https://www.thrive.org.uk/how-we-help/what-we-do/social-therapeutic-horticulture . Accessed 9 Aug 2023.
Cipriani J, Benz A, Holmgren A, Kinter D, McGarry J, Rufino G. A systematic review of the effects of horticultural therapy on persons with mental health conditions. Occup Ther Mental Health. 2017;33:47–69. https://doi.org/10.1080/0164212X.2016.1231602 .
Article Google Scholar
Clatworthy J, Hinds J, Camic PM. Gardening as a mental health intervention: a review. Mental Health Rev J. 2013;18:214–25. https://doi.org/10.1108/MHRJ-02-2013-0007 .
Genter C, Roberts A, Richardson J, Sheaff M. The contribution of allotment gardening to health and wellbeing: a systematic review of the literature. Br J Occup Therapy. 2015;78:593–605. https://doi.org/10.1177/0308022615599408 .
Howarth M, Brettle A, Hardman M, Maden M. What is the evidence for the impact of gardens and gardening on health and well-being: a scoping review and evidence-based logic model to guide healthcare strategy decision making on the use of gardening approaches as a social prescription. BMJ Open. 2020;10: e036923. https://doi.org/10.1136/bmjopen-2020-036923 .
Soga M, Gaston KJ, Yamaura Y. Gardening is beneficial for health: a meta-analysis. Prev Med Rep. 2017;5:92–9. https://doi.org/10.1016/j.pmedr.2016.11.007 .
Spano G, D’Este M, Giannico V, Carrus G, Elia M, Lafortezza R, Panno A, Sanesi G. Are community gardening and horticultural interventions beneficial for psychosocial well-being? A meta-analysis. Int J Environ Res Public Health. 2020;17: 3584. https://doi.org/10.3390/ijerph17103584 .
Lampert T, Costa J, Santos O, Sousa J, Riberio T, Freire E. Evidence on the contribution of community gardens to promote physical and mental health and well-being of non-institutionalized individuals: a systematic review. PLoS ONE. 2021;16:e0255621. https://doi.org/10.1371/journal.pone.0255621 .
Briggs R, Morris PG, Rees K. The effectiveness of group-based gardening interventions for improving wellbeing and reducing symptoms of mental ill-health in adults: a systematic review and meta-analysis. J Mental Health. 2023;32:787–804. https://doi.org/10.1080/09638237.2022.2118687 .
NHS England. Green Social Prescribing. 2022. https://www.england.nhs.uk/personalisedcare/social-prescribing/green-social-prescribing/ . Accessed 9 Aug 2023.
Grantham R, Whaley L. National green social prescribing delivery capacity assessment: final report. London, UK: Department for Health and Social Care, 2023. https://www.gov.uk/government/publications/national-green-social-prescribing-delivery-capacity-assessment/national-green-social-prescribing-delivery-capacity-assessment-final-report . Accessed 21 Aug 2023.
Bragg R, Care Farming. and Green Care Annual Survey 2021: Overview. Social Farms and Gardens. 2021. https://www.farmgarden.org.uk/sites/farmgarden.org.uk/files/gcf_annual_care_farming_green_care_survey_overview_2021.pdf . Accessed 18 Oct 2023.
NHS England. Commissioning Cycle, London UK, England NHS. 2024. https://www.england.nhs.uk/get-involved/resources/commissioning-engagement-cycle/ . Accessed 14 Mar 2024.
Shaw SE, Smith JA, Porter A, Rosen R, Mays N. The work of commissioning: a multisite case study of healthcare commissioning in England’s NHS. BMJ Open. 2013;13:e003341. https://doi.org/10.1136/bmjopen-2013-003341 .
Haywood A, Dayson C, Garside R, Foster A, Lovell R, Husk K, Holding E, Thompson J, Shearn K, Hunt HA, Dobson J, Harris C, Jacques R, Northall P, Baumann M, Wilson I. National Evaluation of the Preventing and Tackling Mental Ill Health through Green Social Prescribing Project: Interim Report Summary – September 2021 to September 2022. London, UK: Department for Environment, Food and Rural Affairs, 2023. https://www.shu.ac.uk/centre-regional-economic-social-research/publications/gsp-interim-report-appendices-sept-2021-to-sept-2022 . Accessed 20 Oct 2023.
Kings Fund. Integrated care systems: how will they work under the health care act? 2022. https://www.kingsfund.org.uk/audio-video/integrated-care-systems-health-and-care-act . Accessed 20 Oct 2023.
Bingham AJ, Witkowsky P. Deductive and inductive approaches to qualitative data analysis. In: Vanover C, Mihas P, Saldaña J, editors. Analyzing and interpreting qualitative data: after the interview. London: SAGE; 2022. p. 133–46.
Google Scholar
Thrive. Therapeutic Horticulture Stakeholder Group. 2023. https://www.thrive.org.uk/how-we-help/therapeutic-horticulturestakeholder-group . Accessed 9 Aug 2023.
Parker C, Scott S, Geddes A. Snowball sampling. In: Atkinson P, Delamont S, Cernat A, Sakshaug JW, Williams RA, editors. SAGE research methods foundations. London: Sage; 2019. https://doi.org/10.4132/9781526421036831710 .
Chapter Google Scholar
Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Res Psychol. 2006;3:77–101. https://doi.org/10.1191/1478088706qp063oa .
Braun V, Clarke V. Thematic analysis. A practical guide. London: Sage; 2022.
Book Google Scholar
NHS England. The long-Term Plan. 2019. https://www.england.nhs.uk/publication/the-nhs-long-term-plan/ . Accessed 21 Aug 2023.
NHS England. ICB running cost allowances: efficiency requirements. 2023. https://www.england.nhs.uk/wp-content/uploads/2023/03/PRN00292-icb-running-cost-allowances-efficiency-requirements.pdf . Accessed 21 Aug 2023.
Rossiter K, Matthews T. National Survey of Gardening and Horticultural Activities for Health & Wellbeing. Reading: Thrive, 2018. https://greencarecoalition.org.uk/national-survey-of-gardening-and-horticulture-related-activities-for-health-and-wellbeing/ . Accessed 25 Oct 2023.
Bragg R, Egginton-Metters I, Leck C, Wood C. Expanding delivery of care farming services to health and social care commissioners. London: Natural England, 2015. https://publications.naturalengland.org.uk/publication/5628503589388288 . Accessed 20 Oct 2023.
Bragg R, Leck C. Good practice in social prescribing for mental health: The role of nature-based interventions. London: Natural England, 2017. https://publications.naturalengland.org.uk/publication/5134438692814848 . Accessed 20 Oct 2023.
The Norfolk Green Care Network. 2023. https://ngcn.uk/ . Accessed 20 Oct 2023.
Reading Green Wellbeing Network. 2023. https://www.rgwn.org.uk/ . Accessed 20 Oct 2023.
Public Health England. A guide to community-centred approaches for health and wellbeing. In: A guide to communitycentered approaches for health and wellbeing. London: Crown; 2015. Accessed 21 Aug 2023.
National Institute for Health and Care Excellence. Community engagement: improving health and wellbeing and reducing health inequalities. London: NICE. 2016. https://www.nice.org.uk/guidance/ng44/resources/community-engagement-improvinghealth-and-wellbeing-and-reducing-health-inequalities-pdf-1837452829381 . Accessed 21 Aug 2023.
Department of Health and Social Care. Major conditions strategy: case for change and our strategic framework. London: Department for Health and Social Care. 2023. https://www.gov.uk/government/publications/major-conditions-strategy-case-for-change-and-our-strategic-framework/major-conditions-strategy-case-for-change-and-our-strategic-framework-2 . Accessed 21 Aug 2023.
Robinson JM, Breed MF. Green prescriptions and their co-benefits: Integrative strategies for public and environmental health. Challenges. 2019;10:9. https://doi.org/10.3390/challe10010009 .
Shanahan DF, Astell–Burt T, Barber EA, Brymer E, Cox DT, Dean J, Depledge M, Fuller RA, Hartig T, Irvine KN, Jones A, Kikillus H, Lovell R, Mitchell R, Niemela J, Mieuwenhuijsen M, Pretty J, Townsend M, van Heezik Y, Warber S, Gaston KJ. Nature–based interventions for improving health and wellbeing: the purpose, the people and the outcomes. Sports. 2019;7:141. https://doi.org/10.3390/sports7060141 .
Tambyah R, Olcoń K, Allan J, Destry P, Astell-Burt T. Mental health clinicians’ perceptions of nature-based interventions within community mental health services: evidence from Australia. BMC Health Serv Res. 2022;22:84. https://doi.org/10.1186/s12913-022-08223-8 .
Claxton R. Gardening4Health Directory. 2020. https://gardening4health.co.uk/ . Accessed 20 Oct 2023.
Fixsen A, Barrett S. Challenges and approaches to green social prescribing during and in the aftermath of COVID-19: a qualitative study. Front. Health Psychol. 2022;13:861107. https://doi.org/10.3389/fpsyg.2022.861107 .
Sempik J, Hine R, Wilcox D. Green Care: A Conceptual Framework. A report of the working group on the health benefits of green care. Loughborough: Centre for Child and Family Research; 2010. https://www.umb.no/statisk/greencare/green_carea_conceptual_framework.pdf . Accessed 20 Oct 2023.
Thrive. Gardening for mental health and wellbeing: consultation document. 2023. https://www.thrive.org.uk/files/documents/THSG-Mapping-V5-for-external-consultation-1.pdf . Accessed 31 Oct 2023.
Wood CJ, Barton JL, Wicks C. The impact of therapeutic community gardening on the wellbeing, loneliness, and life satisfaction of individuals with mental illness. Int J Environ Health Res. 2022;19:13166. https://doi.org/10.3390/ijerph192013166 .
Yang Y, Ro E, Lee TJ, An BC, Hong KP, Yun HJ, Park EY, Cho HR, Yun SY, Park M, Yun YJ, Lee AR, Jeon JI, Jung S, Ahn TH, Jin HY, Lee JL, Choi KH. Multi-sites Trial on the effects of therapeutic gardening on mental health and well-being. Int J Environ Res Public Health. 2022;19:8046. https://doi.org/10.3390/ijerph19138046 .
Buck D. (2016). Gardens for health. Implications for policy and practice. The Kings Fund. https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Gardens_and_health.pdf . Accessed 22 Aug 2023.
The Wildlife Trusts. The Wildlife Trusts’ Natural Health Services. A rapid economic assessment of The Wildlife Trusts’ Natural Health Services. London: The Royal Society of Wildlife Trusts. 2023. https://www.wildlifetrusts.org/sites/default/files/2023-07/23JUN_Health_Report_FINAL%20%281%29.pdf . Accessed 22 Aug 2023.
Wye L, Brangan E, Cameron A, Gabbay J, Klein JH, Pope C. Evidence based policy making and the ‘art’ of commissioning – how English healthcare commissioners’ access and use information and academic research in ‘real life’ decision-making: an empirical qualitative study. BMC Health Serv Res. 2015;15:430. https://doi.org/10.1186/s12913-015-1091-x .
Download references
Acknowledgements
The authors like to acknowledge the funder who enabled this study to take place and the participants for their valuable insights. We would also like to thank the THSG for their help with recruitment of participants to the study.
This work was funded by Research England (grant number FN02200).
Author information
Authors and affiliations.
School of Sport, Rehabilitation and Exercise Sciences, University of Essex, Colchester, CO43SQ, UK
Carly J. Wood, Georgina Morton & Rachel E. Bragg
Thrive, Geoffrey Udall Centre, Beech Hill, Reading, RG72AT, UK
Kathryn Rossiter & Becs Baumber
Rachel Bragg Consultancy, Hereford, HR11GZ, UK
Rachel E. Bragg
You can also search for this author in PubMed Google Scholar
Contributions
CW, KR and RB conceived and designed the study. GM collected, analysed, and interpreted the data. CW also analysed and interpreted the data and drafted the manuscript. GM, KR, BB and RB substantially revised the manuscript. All authors have approved the submitted version.
Corresponding author
Correspondence to Carly J. Wood .
Ethics declarations
Ethics approval and consent to participate.
All participants provided informed consent prior to participation in the study and reconfirmed their consent at the start of the interview. Ethical approval was granted by Ethics Sub-committee 2 at the University of Essex (ETH2223-0519).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Wood, C.J., Morton, G., Rossiter, K. et al. A qualitative study of the barriers to commissioning social and therapeutic horticulture in mental health care. BMC Public Health 24 , 1197 (2024). https://doi.org/10.1186/s12889-024-18621-8
Download citation
Received : 13 November 2023
Accepted : 16 April 2024
Published : 29 April 2024
DOI : https://doi.org/10.1186/s12889-024-18621-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Social and therapeutic horticulture (STH)
- Nature-based intervention (NBI)
- Green social prescribing (GSP)
- Mental illness
- Mental ill-health
- Commissioning
- Mental health
- Health care
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]
Cookies on GOV.UK
We use some essential cookies to make this website work.
We’d like to set additional cookies to understand how you use GOV.UK, remember your settings and improve government services.
We also use cookies set by other sites to help us deliver content from their services.
You have accepted additional cookies. You can change your cookie settings at any time.
You have rejected additional cookies. You can change your cookie settings at any time.
Register to vote Register by 18 June to vote in the General Election on 4 July.
- Health and social care
- Public health
Health trends in England
This report presents trends in data on the health of people in England. Themes covered include risk factors, disease prevalence and outcomes.
Applies to England
https://fingertips.phe.org.uk/static-reports/health-trends-in-england/England/overview.html
The report published on this page, Health trends in England, presents information about the health of people in England and how this has changed over time. Data is presented for England and English regions.
It has been developed by the Department of Health and Social Care and is intended to summarise information and provide an accessible overview for the public. Topics covered have been chosen to include a broad range of conditions, health outcomes and risk factors for poor health and wellbeing. These topics will continue to be reviewed to ensure they remain relevant. A headline indicator is presented for each topic on the overview page, with further measures presented on a detailed page for each topic.
All indicators in health trends in England are taken from a large public health data collection called Fingertips . Indicators in Fingertips come from a number of different sources. Fingertips indicators have been chosen to show the main trends for outcomes relating to the topics presented.
Questions or feedback
If you have any comments, questions or feedback, contact us at [email protected] . Please put ‘Health Trends in England feedback’ as the email subject.
Is this page useful?
- Yes this page is useful
- No this page is not useful
Help us improve GOV.UK
Don’t include personal or financial information like your National Insurance number or credit card details.
To help us improve GOV.UK, we’d like to know more about your visit today. Please fill in this survey (opens in a new tab) .

An official website of the United States government
Here’s how you know
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( A locked padlock ) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Heart-Healthy Living
- High Blood Pressure
- Sickle Cell Disease
- Sleep Apnea
- Information & Resources on COVID-19
- The Heart Truth®
- Learn More Breathe Better®
- Blood Diseases and Disorders Education Program
- Publications and Resources
- Blood Disorders and Blood Safety
- Sleep Science and Sleep Disorders
- Lung Diseases
- Health Disparities and Inequities
- Heart and Vascular Diseases
- Precision Medicine Activities
- Obesity, Nutrition, and Physical Activity
- Population and Epidemiology Studies
- Women’s Health
- Research Topics
- Clinical Trials
- All Science A-Z
- Grants and Training Home
- Policies and Guidelines
- Funding Opportunities and Contacts
- Training and Career Development
- Email Alerts
- NHLBI in the Press
- Research Features
- Past Events
- Upcoming Events
- Mission and Strategic Vision
- Divisions, Offices and Centers
- Advisory Committees
- Budget and Legislative Information
- Jobs and Working at the NHLBI
- Contact and FAQs
- NIH Sleep Research Plan
- Health Topics
- < Back To High Blood Pressure
- Causes and Risk Factors
- What Is High Blood Pressure?
- Living With High Blood Pressure
- Pregnancy and High Blood Pressure
MORE INFORMATION
High Blood Pressure Causes and Risk Factors
Language switcher, what are the risk factors.
Many factors raise your risk of high blood pressure. You can change some risk factors, such as unhealthy lifestyle habits. A healthy lifestyle can lower your risk for developing high blood pressure.
Other risk factors, such as age, family history and genetics, race and ethnicity, and sex, cannot be changed. But, you can still take steps to reduce your risk of high blood pressure and its complications .
Blood pressure tends to rise with age. Blood vessels naturally thicken and stiffen over time. These changes increase the risk for high blood pressure.
However, the risk of high blood pressure is rising for children and teens, possibly because more children and teens have overweight or obesity .
Family history and genetics
High blood pressure often runs in families. Much of what we know about high blood pressure has come from genetic studies. Many genes are linked to small increases in high blood pressure risk. Research suggests that as an unborn baby grows in the womb, some DNA changes may also raise the risk for high blood pressure later in life.
Some people have a high sensitivity to salt in their diet, which can play a role in high blood pressure. This can also run in families.
Lifestyle habits
Lifestyle habits can increase the risk of high blood pressure, including if you:
- Eat unhealthy foods often, especially foods that are high in salt and low in potassium. Some people, including Black people, older adults, and people who have chronic kidney disease, diabetes, or metabolic syndrome, are more sensitive to salt in their diet.
- Drink too much alcohol or caffeine
- Don’t get enough physical activity
- Don’t get enough good-quality sleep
- Experience high-stress situations
- Use substances such as cocaine, methamphetamine, “bath salts,” or other stimulants
Some medicines can make it harder for your body to control your blood pressure. Antidepressants, decongestants (medicines to relieve a stuffy nose), hormonal birth control pills, and non-steroidal anti-inflammatory drugs such as aspirin or ibuprofen can all raise your blood pressure.
Other medical conditions
Other medical conditions change the way your body controls fluids, sodium, and hormones in your blood. Other conditions that can cause high blood pressure include:
- Some tumors
- Chronic kidney disease
- Metabolic syndrome
- Overweight and obesity
- Sleep apnea
- Thyroid problems
Race or ethnicity
High blood pressure is more common in Black adults than in White, Hispanic, or Asian adults. Compared with other racial or ethnic groups, Black people tend to have higher average blood pressure numbers and get high blood pressure earlier in life. Also , some high blood pressure medicines may not work as well for Black people.
During pregnancy , Black women are more likely than White women to develop preeclampsia . Preeclampsia is a pregnancy disorder that causes sudden high blood pressure and problems with the kidneys and liver.
Men are more likely than women to develop high blood pressure throughout middle age. But in older adults, women are more likely than men to develop high blood pressure.
Women who have high blood pressure during pregnancy are more likely to have high blood pressure later in life. Research shows that medicines used to control high blood pressure during pregnancy lower the chance of pregnancy complications and won’t harm the developing baby.
Social and economic factors
Research shows that factors such as income, education level, where you live, and the type of job you have, as well as stressors on the job may raise your risk of high blood pressure. Working early or late shifts is one example of a social factor that can raise your risk.
Experiencing discrimination and poverty has been linked to high blood pressure. Also , some research has shown that experiencing stress, danger, harm, or trauma as a child may raise the risk of high blood pressure.
Can High Blood Pressure be prevented?
How to prevent high blood pressure.
A heart-healthy lifestyle can help prevent high blood pressure and its complications.
- Choose heart-healthy foods that are lower in salt (sodium) and are rich in potassium. Fruits and vegetables are high in potassium. For more ways to limit your sodium, visit the DASH Eating Plan page or print out the Tips to Reduce Salt and Sodium handout.
- Avoid or limit alcohol.
- Get regular physical activity . Even modest amounts can make a difference. Reducing the amount of time you sit each day can help lower your blood pressure.
- Aim for a healthy weight .
- Quit smoking .
- Control your cholesterol and blood sugar levels. To learn some tips to help manage your cholesterol level, read our booklet Therapeutic Lifestyle Changes to Lower Cholesterol .
- Manage stress .
- Get enough good-quality sleep .
- Open access
- Published: 09 May 2024
Factors associated with posttraumatic stress and anxiety among the parents of babies admitted to neonatal care: a systematic review
- Reem Malouf 1 ,
- Sian Harrison 1 ,
- Victoria Pilkington 1 ,
- Charles Opondo 2 ,
- Chris Gale 3 ,
- Alan Stein 4 , 5 , 6 ,
- Linda S. Franck 7 &
- Fiona Alderdice 1 , 8
BMC Pregnancy and Childbirth volume 24 , Article number: 352 ( 2024 ) Cite this article
808 Accesses
8 Altmetric
Metrics details
Posttraumatic stress (PTS) and anxiety are common mental health problems among parents of babies admitted to a neonatal unit (NNU). This review aimed to identify sociodemographic, pregnancy and birth, and psychological factors associated with PTS and anxiety in this population.
Studies published up to December 2022 were retrieved by searching Medline, Embase, PsychoINFO, Cumulative Index to Nursing and Allied Health electronic databases. The modified Newcastle–Ottawa Scale for cohort and cross-sectional studies was used to assess the methodological quality of included studies. This review was pre-registered in PROSPERO (CRD42021270526).
Forty-nine studies involving 8,447 parents were included; 18 studies examined factors for PTS, 24 for anxiety and 7 for both. Only one study of anxiety factors was deemed to be of good quality. Studies generally included a small sample size and were methodologically heterogeneous. Pooling of data was not feasible. Previous history of mental health problems (four studies) and parental perception of more severe infant illness (five studies) were associated with increased risk of PTS, and had the strongest evidence. Shorter gestational age (≤ 33 weeks) was associated with an increased risk of anxiety (three studies) and very low birth weight (< 1000g) was associated with an increased risk of both PTS and anxiety (one study). Stress related to the NNU environment was associated with both PTS (one study) and anxiety (two studies), and limited data suggested that early engagement in infant’s care (one study), efficient parent-staff communication (one study), adequate social support (two studies) and positive coping mechanisms (one study) may be protective factors for both PTS and anxiety. Perinatal anxiety, depression and PTS were all highly comorbid conditions (as with the general population) and the existence of one mental health condition was a risk factor for others.
Heterogeneity limits the interpretation of findings. Until clearer evidence is available on which parents are most at risk, good communication with parents and universal screening of PTS and anxiety for all parents whose babies are admitted to NNU is needed to identify those parents who may benefit most from mental health interventions.
Peer Review reports
Having a baby admitted to a neonatal unit (NNU) can be highly distressing for parents [ 1 , 2 ] and many experience mental health problems during and beyond their baby’s admission [ 3 , 4 , 5 ]. Evidence from a recent systematic review [ 5 ] estimated prevalence of anxiety among parents of babies admitted to NNU was as high as 42% during the first month after birth and remained high at 26% from one month to one year after birth. The prevalence of symptoms of posttraumatic stress (PTS) was equally high at 40% during the first month after birth, 25% from one month to one year and remained high at 27% more than one year after birth.
Unaddressed perinatal mental health problems can have long-term implications for parents, babies and families [ 6 ]. Identifying parents who are at risk of developing mental health problems during this vulnerable time is therefore vital so that timely support and interventions can be delivered [ 7 ]. However, it is unclear why some parents are more susceptible to develop mental health problems and others are more resilient. In the UK, women are asked about their emotional wellbeing routinely at each antenatal and postnatal contact with healthcare professionals [ 8 ]. For women in the general perinatal population, a number of factors are associated with perinatal anxiety. Obstetric factors include current or previous pregnancy complications, surgical obstetric interventions, and miscarriages; health and social factors include a history of mental health problems, domestic violence, being a single parent, having a poor couple relationship or inadequate social support [ 9 , 10 , 11 , 12 ]. PTS is associated with traumatic birth events including changes to birth plan, birth before arrival to hospital, emergency caesarean birth, instrumental vaginal birth, and manual removal of the placenta; third and fourth-degree perineal tears are additional risk factors for PTS after birth [ 13 , 14 ]. The experience of childbirth in and of itself is an independent factor associated with PTS and therefore preterm birth and neonatal complications are considered as add-on stressors [ 15 ].
The factors associated with developing postnatal mental health problems in parents of babies admitted to NNU have received comparatively little attention and are poorly understood. It is unclear whether the factors associated with increased risk of mental health problems in the general perinatal population are applicable to parents of babies admitted to NNU, or whether there are different or additional factors for this population. Factors such as the unexpected nature of many NNU admissions, separation from the newborn, and concern about the infant’s health make the experience of parents with babies receiving neonatal care different from that of other parents. Therefore, it is important to understand the risk and protective factors for this specific population to ensure that approaches for assessment, detection and intervention for perinatal mental health problems are optimally delivered and, if necessary, appropriately tailored.
The aim of the review was to systematically collate, appraise and synthesise the current evidence on risk and protective factors for developing PTS and anxiety in parents of babies admitted to NNU.
Operational definitions
There is no formal or internationally agreed definition of NNUs. The UK Department of Health and Social Care’s definition includes special care units (SCUs), local neonatal units (LNUs) and neonatal intensive care units (NICUs) [ 16 ]. The American Academy of Paediatrics’ definition of NNUs include basic care (level I), specialty care (level II), and subspecialty intensive care (level III, level IV) [ 17 ]. Within the context of this review we included studies on parents of babies admitted to any level of NNU.
The Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) [ 18 ] defines anxiety disorders as disorders that share features of excessive fear and anxiety and related behavioural disturbance. PTS is associated with exposure to trauma. Acute Stress Disorder (ASD) occurs within four weeks of a traumatic event, while Posttraumatic Stress Disorder (PTSD) occurs when symptoms persist beyond one month. Throughout this review, the term ‘PTS’ is used to cover clinically significant ASD, PTSD or PTS symptoms and the term ‘anxiety’ is used to cover both clinically significant anxiety symptoms or disorders.
The review protocol was prospectively registered with PROSPERO (CRD42021270526) and reporting followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [ 19 ].
Eligibility criteria
Studies published in any language which examined the potential association of at least one risk factor with PTS or anxiety and were conducted with parents (mothers, fathers and carers) of babies admitted to any level of a NNU in all countries were included. Studies focusing on specific groups such as parents with existing mental health conditions or parents of deceased babies were also considered for inclusion. All observational study designs were eligible.
Search strategy and selection criteria
A comprehensive search strategy was developed and tested using a combination of free-text (title/abstract) keywords and MeSH subject terms to describe the key concepts of PTS/anxiety, parents and NNUs. The search covered the period from the inception of each database until December 2022. No restriction was applied to the electronic searches. The following databases were searched: Medline, Embase, PsychoINFO, Cumulative Index to Nursing and Allied Health literature, Web of Science, ResearchGate and Google Scholar; Grey literature was also searched including Ethos, Proquest Dissertations & Theses and OpenGREY. The reference lists of all included studies were also searched for additional eligible studies. The search strategy applied in Medline is shown in Appendix 1 .
Study selection and data extraction
All screening of titles, abstracts and full texts was conducted in Covidence [ 20 ]. A data extraction form was piloted on selected studies and was then employed for the remaining studies. Data on country, study design, aims, inclusion/exclusion criteria, characteristics of included parents and babies, PTS/anxiety measuring tools, assessment time, potential risk and protective factors relevant to PTS and anxiety, data analysis method and estimated effects for each risk factor were extracted. All screening and data extraction were independently performed by at least two reviewers (RM, VP, SH, FA). Any discrepancies were discussed and resolved by a third author (FA, SH). Authors were contacted when required information was missing or when full texts were not available ( N = 16).
Risk of bias assessment
The quality and certainty of evidence were assessed using a modified version of the Newcastle–Ottawa Scale [ 21 ]. The modified tool contains seven domains of bias relating to the following sources: selection, sampling, measurement of factors/outcome, analysis, selective reporting and attrition. Low, high or unclear risk rating was used to assess the potential bias for each domain.
Data synthesis
Summary statistics were extracted from all studies, including number of participants, number of risk factors and data relevant to each risk factor identified. When results from univariable and multivariable analyses were reported, only the latter were extracted. Meta-analyses by exposures/risk factors were not feasible due to the variability in the measurement of similar risk factors across studies (e.g. type of measurement tool, cut-off point, categorical or continuous data). Therefore, results were narratively synthesized and reported for PTS and anxiety separately.
A total of 6,662 records were identified and, after removing duplicates, 3,788 records were screened, of which 3,615 records were excluded. 162 reports were assessed for full-text eligibility (11 reports could not be retrieved) and, of these, 110 reports were excluded with reasons and 49 studies, published in 52 records, were included. 18 studies, published in 19 records, reported on factors associated with PTS, 24 studies on anxiety and 7 studies, published in 9 records, reported on both, see Fig. 1 .

PRISMA flow chart of study selection
Post-traumatic stress (PTS)
Description of the included studies.
Table 1 presents the 25 studies published in 28 records [ 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 ] for PTS (including 7 studies reporting both PTS and anxiety). More than half of the studies were conducted in the USA [ 22 , 25 , 27 , 28 , 29 , 30 , 31 , 34 , 35 , 41 , 42 , 44 , 45 , 46 , 47 ], five in Europe, published in six records [ 23 , 26 , 36 , 37 , 48 , 49 ] two in Canada [ 32 , 43 ], and one in each of the following countries: Australia [ 39 ], Argentina [ 40 ], Iran [ 38 ], South Korea [ 50 ] and Taiwan [ 24 ]. Six studies [ 24 , 25 , 27 , 41 , 44 , 47 ] were of a cross-sectional design and the remaining studies were cohort studies.
Two studies included bereaved parents of babies who had been admitted to NNU [ 25 , 30 ] and one study [ 22 ] focused entirely on military families. Both parents were included in ten studies, published in 11 records [ 22 , 25 , 30 , 34 , 35 , 38 , 39 , 42 , 46 , 47 , 48 ] and only mothers were enrolled in the remaining studies. Gestational age (GA) of the infant was an inclusion criterion in nine studies published in ten records [ 23 , 24 , 26 , 32 , 36 , 37 , 38 , 39 , 43 , 45 ], and birth weight (BW) was a criterion in two studies published in three records [ 28 , 29 , 31 ]. Two studies included both GA and BW in their inclusion criteria [ 27 , 40 ]. All studies used standardised self-report scales.
None of the included studies were at low risk of bias across all domains (see Fig. 2 - A summary of risk of bias of PTS studies and Appendix 2 ). All studies had high risk of selection bias because all applied some exclusion criteria and most used convenience sampling. Ten studies, published in 12 records [ 23 , 25 , 28 , 29 , 32 , 36 , 37 , 42 , 43 , 45 , 48 , 49 ], did not employ adequately powered sample sizes. Twelve studies [ 23 , 26 , 27 , 31 , 32 , 38 , 40 , 41 , 42 , 44 , 47 , 49 ] had high risk of analysis bias due to unmeasured confounding factors or correlational analysis only, and seven studies [ 22 , 23 , 24 , 25 , 31 , 42 , 47 ] had high risk of attrition bias due to low participation rates or high loss to follow-up. All except two studies [ 40 , 47 ] had low risk of reporting bias. All studies were at low risk of bias for factor and outcome measurement.

Risk of bias summary of post-traumatic (PTS) included studies
Factors associated with post-traumatic stress (PTS)
Overall, 2,506 parents were involved across the 25 included studies with sample sizes ranging from 29 to 245 participants. A total of 62 potential risk or protective factors were identified. The factors are detailed in Table 2 , presented in a mapping diagram in Table 3 and summarised here under the following eight categories: parent demographic factors; pregnancy and birth factors; infant demographic factors; infant health factors; parent history of mental health symptoms; parent postnatal psychological factors; parent stress and coping, and other factors.
1) Parent demographic factors (Ten factors: age, education, sex, ethnicity, parents’ area deprivation, income, employment status, housing and access to transport, single parent, family social risk)
The association between parental age and PTS symptoms was explored in nine studies, published in ten records [ 23 , 27 , 29 , 33 , 34 , 36 , 37 , 40 , 43 , 46 ]. Older mothers had significantly higher PTS scores at two weeks post NNU admission in one study of only 29 mothers, reported in two records [ 36 , 37 ]. In the remaining studies there was no significant association between parental age and PTS symptoms. Seven studies [ 23 , 25 , 27 , 33 , 40 , 43 , 46 ] explored the association between parental education and PTS symptoms. Lower education was associated with more PTS symptoms in three studies [ 25 , 40 , 43 ] and consistent with this finding, one study [ 43 ] found mothers with more years of education had fewer PTS symptoms at discharge. Similarly, in another study [ 40 ], mothers who had a lower education level accounted for significantly more cases of PTS at 6–36 months after birth. Additionally, among bereaved mothers [ 25 ], higher education level was associated with fewer PTS symptoms even three to five years after the baby’s death. The remaining four studies found no association between parental education and PTS symptoms. The association between sex of parent and PTS symptoms was explored in seven studies [ 22 , 25 , 34 , 38 , 39 , 42 , 47 ]. Three studies [ 34 , 38 , 39 ] provided data at multiple time points. Two studies [ 38 , 47 ] found PTS symptoms were significantly more prevalent in mothers than fathers while their babies were still in NNU and a month later [ 38 ]. Evidence from the remaining five studies showed no association between sex of parent and PTS symptoms. Three studies [ 34 , 46 , 47 ] explored the association between parental ethnicity and PTS symptoms, and none found any association during NNU stay [ 34 , 47 ] or at three months post NNU discharge [ 46 ]. However, in one of the studies [ 34 ], only 28% of participants were from minority backgrounds. The association between parents’ area deprivation and PTS was explored in one study [ 29 ], and mothers residing in poorer neighbourhoods had lower PTS scores at birth than those residing in more privileged neighbourhoods, but this association disappeared at one year. Housing and access to transport were not associated with PTS symptoms at three months post NNU discharge in one study [ 46 ]. In bereaved parents [ 25 ], a lower family income for fathers, but not for mothers, was significantly associated with more PTS symptoms at three months to five years after the baby’s death. Two studies [ 38 , 46 ] explored the association between employment status and PTS symptoms. One study [ 46 ] found employment status was not associated with PTS symptoms after birth, yet the other study [ 38 ] found PTS symptoms were significantly greater among employed mothers and mothers with unemployed partners one month after the birth [ 38 ]. One study [ 35 ] found no significant association between being a single parent and PTS symptoms three months after NNU discharge. One study [ 39 ] explored family social risk, a composite of family structure, education, occupation, employment, language spoken and maternal age, and found no association with PTS symptoms in parents of very preterm infants at 12 and 24 months corrected age.
2) Pregnancy and birth factors (Seven factors: parity, multiple pregnancy, mode of birth, pre-eclampsia, threatened preterm labour, in-vitro fertilisation, traumatic childbirth)
Three studies [ 23 , 28 , 33 ] explored the association between parity and PTS symptoms. Two of the studies [ 28 ] found primiparity was a significant risk factor for elevated PTS symptoms during NNU [ 25 ] and at one year corrected age [ 33 ] and the third study [ 23 ] found no significant association between parity and PTS symptoms 18 months after birth. Multiple pregnancy was explored in three studies [ 23 , 33 , 39 ] and giving birth to twins was not associated with PTS symptoms in any study assessed at one year or later. The association between mode of birth and PTS symptoms was explored in two studies, reported in three records [ 23 , 36 , 37 ]. One study, reported in two records (2013, 2014), found planned caesarean section compared to normal birth was associated with lower PTS symptom scores at two weeks post NNU admission. However the other study [ 23 ] found caesarean section (planned and unplanned) was not significantly associated with PTS symptoms at 18 months, yet there were more caesarean sections among the group of mothers who experienced PTS symptoms during the study. Seventy-five percent required a caesarean section compared to 47.4% in the group with no significant PTS symptoms. Preeclampsia was significantly associated with higher PTS scores at two weeks post NNU admission in one study, reported in two records [ 36 , 37 ]. A history of threatened preterm labour was explored in one study [ 23 ] and was not associated with PTS symptoms at 18 months after birth. In vitro fertilization [ 23 ] and traumatic childbirth [ 41 ] were each explored in one study and were not found to be associated with PTS symptoms at one to four months and 12 months after birth, respectively.
3) Infant demographic factors (Five factors: gestational age, birth weight, Apgar score, sex of infant, age at infant)
Seven studies [ 22 , 23 , 33 , 40 , 42 , 43 , 46 ] explored the association between gestational age (GA) and PTS symptoms. Only two studies [ 23 , 40 ] found a significant association between GA and PTS symptoms. One study [ 23 ], where GA ≤ 32 weeks was an inclusion criterion, found that infants born to mothers with elevated PTS scores 18 months after birth had a lower GA age by almost one week, and one study [ 40 ] found a significantly higher frequency of infants born ≤ 28 weeks gestation among mothers with more PTS symptoms 6 to > 36 months after birth. The association between birth weight (BW) and PTS symptoms was explored in five studies, [ 23 , 26 , 29 , 40 , 42 ]. Increased infant’s BW was significantly correlated with lower PTS symptoms during NNU stay [ 26 ] and lower PTS score at birth, but not at 12 months later [ 29 ]. PTS symptoms were more prevalent at six to > 36 months among mothers to a very low BW (< 1000 g) infant [ 40 ]. Two other studies [ 23 , 42 ] reported no significant association between BW and PTS symptoms at four and 18 months after birth, respectively. The association between Apgar score and PTS symptoms was explored in four studies [ 23 , 33 , 42 , 44 ] and only one study [ 44 ] found Apgar scores (1 min, 5 min) and PTS symptoms were negatively correlated during NNU admission. Two studies explored sex of infant and PTS symptoms and found no association at NNU discharge [ 43 ] or 18 months after birth [ 23 ]. One study explored age of infant and PTS symptoms at 7–24 months vs 25 to > 36 months and found no association [ 40 ].
4) Infant health and care factors (17 factors: clinicians’ perception of infant health, parents’ perception of infant health, mother-infant contact, length of NNU stay, mother-infant relationship, mother-nurse relationships, hypoxic ischemic encephalopathy (HIE), ventilation, severe bronchopulmonary dysplasia, vasopressor, hypoxic ischemic encephalopathy (HIE), palliative care consultation, seizures, invasive procedures, number of medical interventions, infant general development, re-hospitalisation and emergency visit.
Nine studies reported on clinicians’ perception of infant health [ 23 , 25 , 26 , 27 , 34 , 35 , 40 , 44 , 49 ]. Three studies [ 23 , 26 , 49 ] used the Perinatal Risk Inventory (PERI) scale [ 51 ] to assess clinicians’ perceived risk of adverse infant outcomes. One study [ 26 ] found a significant correlation between PRI score and parental PTS symptoms during NNU, one study found a significant correlation during NNU admission but not 12 months later [ 49 ], and one study found no association at 18 months corrected age [ 23 ]. One study used the Neonatal Acute Physiology-Perinatal Extension- II (SNAPPE-II) [ 44 ], a tool for predicting outcomes in critically ill newborns, and found a significant correlation between SNAPPE-II scores and PTS symptoms during NNU admission. Four studies [ 25 , 34 , 35 , 40 ] used non-standardised clinical indicators to assess clinicians’ perception of the baby’s health but only one study reported a significant association. In one study [ 40 ], severe neonatal morbidity was significantly more common among mothers with elevated PTS score 6—> 36 months after birth. However, the Neurobiologic Risk Score (NBRS) [ 52 ] which assesses baby’s neurological insults was not significantly correlated with PTS scores three months after birth [ 27 ].
The association between parents’ perception of infant health and PTS symptoms was assessed in five studies, published in six records [ 22 , 25 , 35 , 44 , 45 , 46 ], and all studies reported a significant association. Parents who appraised their infant’s health as “sick/severe” were almost four times more likely to report PTS symptoms in two studies, one at 1–2 months [ 22 ] and one at three months post NNU discharge [ 35 ]. Also in [ 46 ], parents’ uncertainty about infant’s health was significantly associated with higher PTS scores during NNU and at three months post discharge. Among parents of deceased babies [ 25 ], mothers’ perception of infants’ symptoms and fathers’ perception of infants’ suffering were associated with increased PTS scores even three to five years following infant death. One study found a significant correlation between subjective infant health and more PTS symptoms during NICU admission [ 44 ] and one study found that a higher number of health problems reported by the mother was associated with higher PTS scores six months after birth [ 45 ]. Neither mother-infant contact (verbal and physical contact rated on a five-point Likert scale) while in NNU nor the number of NNU visits per week were associated with PTS symptoms at six months [ 45 ]. Additionally, mother-infant relationship assessed by CARE-index [ 53 ], which measures the interaction patterns between infants and carers, was not associated with more PTS symptoms during NNU stay or at 12 months corrected age [ 49 ]. One study explored mother-nurse relationships at six months [ref],based on nurses rating mothers’ understanding of explanations relating to infants’ care and health (,and found no association with PTS scores.
Length of stay in NNU was explored in seven studies [ 34 , 40 , 41 , 42 , 43 , 45 , 46 ] and only one study [ 43 ] adjusted for GA. Three studies [ 34 , 45 , 46 ] found significant, albeit contradictory, associations between length of NNU stay and PTS symptoms. One study [ 34 ] found longer length of stay was correlated with lower PTS scores during NNU admission and two studies [ 45 , 46 ] found longer length of stay was associated with higher PTS scores at three months [ 46 ] and six months [ 45 ]. Low grade intraventricular haemorrhage (IVH) was significantly associated with higher PTS scores 2 weeks after NNU admission in one small study, reported in two records [ 36 , 37 ]. Requiring ventilation for > 30 days, severe bronchopulmonary dysplasia (BPD) and vasopressors support were all more prevalent among parents who reported PTS at three months post NNU discharge [ 46 ] in one study. Parents of infants exposed to a greater number of invasive procedures had significantly more PTS symptoms during NNU in one study [ 43 ] which adjusted for GA. Conversely, another study [ 25 ] found number of medical interventions was not significantly associated with PTS symptoms 3 months to 5 years after infant death. Hypoxic ischemic encephalopathy (HIE), palliative care consultation and seizures were not associated with PTS scores in one study [ 46 ]. One study explored infant’s general development [ 49 ] and one study explored rehospitalisation or emergency visits [ 33 ]; neither were found to be significantly associated with PTS symptoms.
5) Parental history of mental health/trauma factors (Four factors: parental history of mental health problems, family history of mental health problems, previous traumatic events, traumatic childbirth).
Three studies reported on parental history of mental health problems [ 22 , 45 , 46 ] and all found significant associations. One study [ 22 ] found a significant association with a positive screening of PTS two weeks after birth, one study found an association during NNU [ 45 ] and at three months post NNU discharge [ 46 ]. One study found [ 45 ] previous mental health problems in addition to low mother-infant contact (physical or verbal) was significantly associated with higher PTS scores during NICU admission. Two studies [ 34 , 46 ] reported a significant association between family history of depression/mental health problems and PTS symptoms during NNU admission [ 34 ] and at three months post discharge [ 46 ]. Previous traumatic events (physical or psychological e.g. car accident, unexpected death of loved ones and sexual assaults) were assessed in three studies, published in four records [ 28 , 29 , 38 , 41 ] with mixed results. One study, published in two records [ 28 , 29 ], found exposure to previous traumatic events was associated with increased PTS scores at birth and before NNU discharge, but not at one year. One study [ 38 ] found that a history of traumatic events, during recent years was not associated with PTS symptoms three to five days after birth, but was associated with PTS among mothers at a later assessment point around one month after birth. Finally, one study [ 41 ] found that prior trauma exposure was not associated with a significant increase in PTS scores one to four months after birth. PTS symptoms were higher among women who had a traumatic childbirth compared with those who did not, but no significant association was found in the regression analysis [ 41 ].
6) Parental postnatal mental health factors (Four factors: postnatal depression, postnatal anxiety, early PTS symptoms, other mental health problems)
The association between postnatal depression and PTS was explored in seven studies [ 22 , 23 , 26 , 31 , 32 , 42 , 48 ]. The timing of the assessment varied across the studies: during NNU admission [ 26 , 31 , 32 , 42 ], at discharge [ 22 , 23 , 26 , 32 ], four months after birth [ 42 ] or at one year post discharge among fathers [ 48 ]. All studies reported a significant association between postnatal depression and PTS symptoms irrespective of when the measurement was taken.
The association between postnatal anxiety and PTS was explored in five studies [ 23 , 26 , 27 , 31 , 47 ]. All reported a significant correlation between anxiety scores and PTS scores during NNU admission [ 26 , 31 , 47 ], at three months after birth [ 27 ] and at 18 months after birth [ 23 ]. In four studies [ 22 , 34 , 42 , 45 ], the association between early PTS symptoms and PTS symptoms later in the postnatal period was explored. PTS symptoms around the time of NNU admission was a significant risk factor for an increase in PTS symptoms at one month post discharge [ 34 ], at 1–2 months post discharge [ 22 ] and 4 months after birth [ 42 ]. However, PTS scores during NNU stay were not significantly associated with PTS scores at 6 months [ 45 ].
Other mental health symptoms were explored in three studies [ 24 , 26 , 42 ]. The combination of anxiety and depression assessed by the Hospital Anxiety and Depression Scale (HADS) was correlated with PTS around birth and before NNU discharge in one study [ 26 ]. The combination of high depression and neuroticism scores was a significant risk factor for PTS at six to 48 months after birth in one study [ 24 ]. Finally, general psychiatric symptomatology assessed by the Symptom Checklist-90–Revised (SCL-90–R) was significantly correlated with PTS scores in another study [ 42 ].
7) Parent stress, coping and support factors (11 factors: Parental Stressor Scale total score, stress related to infant’s appearance, stress related to sights and sounds, stress related to parental role alteration, stress related to parent-staff relationships, concurrent stressors, forward-focused coping style, maternal optimism, worry about infant’s death, social support, psychological support).
Parental stress was measured using the Parental Stressor Scale: Neonatal Intensive Care Unit (PSS: NICU) [ 54 ] in four studies [ 31 , 41 , 42 , 48 ]. The PSS: NICU assesses different domains of stress including sights and sounds, infant appearance and parental role in addition to providing a total parental stress score. Examples of stress related to alteration in the parental role are feeling helpless, being separated from the infant and unable to provide care. Three studies [ 41 , 42 , 48 ] reported PSS total scores; two studies found a significant association with an increase in PTS scores at one to four months after birth [ 41 ] or at one year after NNU discharge [ 48 ]. However, another study found no association was reported at four months after birth [ 42 ]. Two studies [ 31 , 42 ] reported on parental stress related to infant’s appearance and this was associated with higher PTS scores in one study [ 31 ] when PTS was assessed on admission to NNU; another study found no significant association when PTS was measured at 4 months [ 42 ]. One study [ 42 ] found PTS scores were significantly correlated with the stress related to sights and sounds in the NNU at four months post birth. Stress related to role alteration during NNU admission was evaluated in three studies [ 22 , 31 , 42 ], only one of which found higher stress relating to role alteration correlated with higher PTS scores during NNU admission [ 31 ]. One study [ 42 ] found that stress relating to relationships with staff during NNU was not significantly correlated with PTS scores.
The number of concurrent stressors was found to be a significant risk factor during NNU admission in one study [ 34 ]. Concurrent stressors included social stressors, such as change in relationship status, living arrangements, or job status, and stressors such as loss, personal or family health concerns, experience of a traumatic event or legal problems.
Coping styles and flexibility after a traumatic event were assessed in one study [ 45 ] using the perceived ability to cope with trauma scale [ 55 ], which has two subscales: forward focus and trauma focus. A forward-focused coping style was not associated with PTS symptoms [ 45 ], whereas maternal optimism about the infant’s recovery while in NNU significantly reduced the likelihood of reporting PTS at 6 months [ 45 ]. One study explored worry about infant’s death and found it was not associated with PTS during NNU admission [ 44 ]. Two studies looked at the association between social support and PTS symptoms [ 26 , 48 ]. Satisfaction with social support was associated with lower PTS symptoms in one study [ 26 ] and maternal social functioning was associated with a reduction in PTS at one year after NNU discharge in another study [ 48 ]. Mothers scoring above and below the cut-off point on the modified perinatal PTSD questionnaire were not found to differ in the psychological support they received in a further study [ 23 ].
8) Other factors (Four factors: geographic separation, active duty, spiritual activities, religious activities)
In a study including military personnel [ 22 ], geographic separation (defined as a combat zone deployment of any duration and a separation from family for more than four months at any time, or for more than one month during the most recent pregnancy) and active military service of either parent was not significantly associated with PTS at any time point. In a study of bereaved parents [ 30 ], spiritual activity without adopting a specific religion was associated with lower PTS scores among mothers but not fathers, whereas using religious activities as a coping mechanism was not associated with a significant reduction in PTS scores in either parent.
Description of included studies
Table 4 presents the 31 included studies, published in 33 records [ 27 , 28 , 29 , 31 , 36 , 37 , 45 , 49 , 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 , 66 , 67 , 68 , 69 , 70 , 71 , 72 , 73 , 74 ], for anxiety (including 7 studies for both anxiety and PTS).
Twelve studies, published in 13 records, came from USA [ 27 , 28 , 29 , 31 , 45 , 47 , 57 , 64 , 67 , 69 , 70 , 76 , 78 ]. Six studies, published in seven records, were from Europe [ 36 , 37 , 49 , 56 , 58 , 59 , 72 ]. Two studies were from Brazil [ 62 , 66 ] and two from Australia [ 71 , 75 ], and one was from each of the following countries: New Zealand [ 68 ], Canada [ 65 ], China [ 74 ], Korea [ 79 ], Iran [ 63 ], Turkey [ 60 ], Tunisia [ 73 ] and India [ 77 ].
Eight studies involved both parents [ 47 , 58 , 65 , 68 , 72 , 74 , 75 ], one either parents [ 76 ],one [ 59 ] included only fathers, and the remaining 21 studies included only mothers. One study only included mothers of babies with congenital anomalies [ 66 ], two studies [ 71 , 72 ] compared multiples to singletons and one study [ 71 ] compared bereaved to non-bereaved parents.
GA of the infant was an inclusion criterion in 17 studies, published in 18 records [ 27 , 36 , 37 , 45 , 49 , 56 , 58 , 61 , 62 , 63 , 65 , 67 , 68 , 69 , 71 , 75 , 76 , 79 ], and BW was a criterion in eight studies, published in nine records [ 27 , 28 , 29 , 31 , 61 , 65 , 67 , 68 , 71 ]. One study [ 72 ] used both GA and BW to define preterm infants. The studies used various measures of general anxiety symptoms.
One study [ 56 ] was rated at low risk of bias across all domains (See Fig. 3 -A summary of risk of bias of anxiety studies and Appendix 3 ). In the remaining studies, sample selection bias was low in two studies only [ 65 , 68 ]. Bias due to sample size was low in 14 studies [ 27 , 31 , 47 , 56 , 57 , 60 , 63 , 65 , 68 , 70 , 71 , 74 , 75 , 77 ]. All except one study [ 59 ] used valid measures to assess the factors. Anxiety was assessed via standardised measures in all studies. The bias in the analysis domain was low in eleven studies, published in thirteen records [ 28 , 29 , 36 , 37 , 45 , 56 , 59 , 64 , 67 , 71 , 74 , 76 , 78 ]. Reporting bias was low in all except five studies [ 47 , 62 , 63 , 69 , 78 ] and attrition bias was low in all except in eight studies where it was high [ 31 , 57 , 61 , 65 , 67 , 70 , 75 , 76 ] and unclear in four [ 62 , 73 , 74 , 78 ].

Risk of bias summary of anxiety included studies
Factors associated with anxiety
Overall, 5,941 parents were involved across the 31 included studies with sample sizes ranging from 29 to 2270 participants. A total of 73 potential risk factors were identified. The risk factors are detailed in Table 5 , mapped in Table 6 , and summarised here using the same eight categories as for PTS.
1) Parent demographic factors (11 factors: age, education, sex, couple’s relationship, family income, employment, ethnicity, residential area, medical insurance, smoking, cumulative psychosocial risk factors).
1) Parent demographic factors (Ten factors: age, education, sex, ethnicity, parents’ area deprivation, income, employment status, housing and access to transport, single parent, family social risk).
Parental age was examined as a determinant of anxiety in eight studies [ 27 , 56 , 62 , 63 , 69 , 70 , 74 , 79 ] and none showed any significant association with developing anxiety at any time point. The association between parental education and anxiety was reported in eight studies [ 27 , 28 , 61 , 62 , 63 , 70 , 74 , 79 ]. In one study [ 61 ], parents’ educational level correlated negatively with anxiety scores and in another study [ 74 ], parents with low education levels had significantly higher anxiety scores. In contrast, in one study [ 63 ], mothers with university degrees had higher state anxiety scores after birth compared to mothers with a diploma or lower level of educational attainment. No evidence of association between elevated anxiety scores and parental factors was found in the remaining studies.
The association between sex of parents and anxiety was reported in seven studies [ 47 , 58 , 65 , 68 , 72 , 74 , 75 ]. In two studies [ 47 , 68 ], fathers reported significantly fewer anxiety symptoms than mothers during NNU admission [ 47 ] and also at nine months [ 68 ]. In all other studies, no significant associations were found. Couple’s relationship was explored in five studies [ 56 , 59 , 62 , 69 , 70 ]. Being married was associated with lower anxiety scores during NNU admission in one study [ 70 ], yet marital status was not associated with anxiety symptoms in the other three studies [ 56 , 62 , 69 ]. A negative description of a couple’s relationship status was associated with greater anxiety scores in fathers two to three weeks after birth in one study [ 59 ].
The relationship between family income and anxiety was investigated in six studies [ 29 , 59 , 62 , 63 , 70 , 74 ]. In one study, having a low income status was associated with lower anxiety scores amongst mothers at the time of birth [ 29 ]. In contrast, in another study, low family income was associated with elevated paternal anxiety symptom scores after birth [ 59 ]. In four studies [ 62 , 63 , 70 , 74 ] family income was not significantly correlated with anxiety scores. Employment was explored in five studies [ 56 , 59 , 63 , 70 , 79 ]. An unemployed father was associated with elevated anxiety scores among fathers at birth in one study [ 59 ]. However, in the four other studies, no association was found between parents’ employment status and developing anxiety at birth [ 63 ], two to three weeks after birth [ 79 ], during NNU admission [ 70 ] or at NNU discharge [ 56 ]. Three studies [ 47 , 69 , 70 ], considered ethnicity as a factor relevant to anxiety during NNU stay and no significant association was found. Area deprivation was evaluated in relation to anxiety in two studies [ 74 , 76 ]: parents residing in more economically advantaged areas were found to be 6.5 times more likely to report anxiety two weeks after birth during the NNU stay [ 76 ]. Anxiety scores during the first week after birth were lower among mothers living in an urban residential area compared to those living in a rural area [ 74 ], and the same study found higher anxiety scores among women without medical insurance compared to those who were insured [ 74 ]. One study explored smoking status and found that smoking was not significantly correlated with anxiety [ 69 ]. One study [ 78 ] looked at a cumulative psychosocial risk factor score, comprising younger maternal age, perceived stress and low socio-economic status),- and found this was significantly associated with greater maternal anxiety scores.
2) Pregnancy and birth factors (15 factors: parity, in-vitro fertilisation, multiple pregnancy, number of antenatal visits, preeclampsia, pregnancy complications, cumulative obstetric risks, mode of birth, preterm birth, infant health risk/congenital anomalies, timing of when parents met their newborn, skin to skin, postnatal care education, mother’s length of stay, maternal severe morbidity).
The association between parity and anxiety was explored in nine studies [ 28 , 37 , 56 , 59 , 61 , 62 , 63 , 69 , 79 ]. Being primiparous, a first time mother, was an independent risk factor associated with anxiety in four studies [ 28 , 37 , 59 , 79 ]. Primiparous mothers had significantly higher anxiety scores than multiparous mothers at two to three weeks after birth [ 79 ]. Similarly, primiparous mothers were seven times more likely to report anxiety symptoms prior to NNU discharge [ 28 ]. Even when the assessment was at six to eighteen months post term, primiparity was still a significant risk factor for state anxiety [ 37 ]. However, being primiparous was not associated with state anxiety symptoms at NNU discharge in two studies [ 56 , 69 ]. In two further studies, multiparous compared to nulliparous mothers exhibited higher state anxiety scores [ 61 , 63 ]. Furthermore, mothers who had given birth three or more times had higher state and trait anxiety mean scores in one study [ 63 ]. No correlation was reported between number of children and anxiety during NNU stay or at discharge [ 62 , 69 ]. Among fathers [ 59 ], a significant association was found between being a first time father and elevated state anxiety scores after birth. Assisted reproductive techniques [ 59 , 79 ], multiple pregnancy [ 56 , 59 , 71 , 72 , 79 ], number of antenatal visits [ 62 ], and preeclampsia were not significant risk factors for state anxiety at NNU discharge [ 56 ]. However, pregnancy complications were significantly correlated with elevated state and trait anxiety scores during NNU stay [ 62 ]. A cumulative obstetric risk score comprising preeclampsia, high blood pressure and diabetes was not associated with higher anxiety scores in one study [ 78 ]. Mode of birth was considered in five studies [ 56 , 59 , 62 , 63 , 77 ]. Having a caesarean section after 26 weeks was associated with more state anxiety symptoms compared to spontaneous vaginal birth after 26 weeks, evidence from a large study that adjusted for neonatal birthweight, severe neonatal morbidity, maternal age, employment and parity [ 56 ]. No association was found in the remaining four studies [ 59 , 62 , 63 , 77 ]. Preterm birth, either induced or spontaneous, was not associated with developing state anxiety at NNU discharge in one good quality study [ 56 ]. Two studies looked at the influence of receiving information about health risk or congenital anomaly in the foetus during antenatal scans on anxiety. Among fathers [ 59 ], infant health risks detected antenatally were a significant risk factor for anxiety at two–three weeks post birth. However, among mothers, trait anxiety was lower when baby’s diagnosis of congenital anomalies was made antenatally than postnatally [ 66 ]. Timing of when parents met their newborn [ 56 ], skin to skin contact, [ 56 ], receiving postnatal care education [ 79 ], mothers’ length of hospitalisation [ 59 ] and a composite factor of severe maternal morbidity [ 56 ] were not significantly associated with anxiety.
3) Infant demographic factors (Six factors: gestational age, birthweight, prematurity, Apgar score, sex, cumulative neonatal risk factor)
Gestation age was considered in seven studies [ 37 , 59 , 62 , 63 , 70 , 77 , 79 ]. Mothers to infants born at 33 weeks of gestational age or less experienced higher state anxiety at birth compared to mothers > 34 weeks [ 63 ] and at two to three weeks after birth [ 79 ]. This was consistent even at a later assessment at six and 18-month post-term age [ 37 ]. Among fathers, GA ≤ 28 week vs > 28 was not a significant factor associated with higher state anxiety scores after birth or 2–3 weeks later [ 59 ], nor was GA < 37 and ≥ 37 weeks among mothers [ 77 ]. Birth weight was reported in eight studies [ 29 , 59 , 61 , 62 , 63 , 70 , 73 , 77 ]. Lower BW was significantly correlated with higher anxiety scores in one study [ 61 ]. Moreover, each 100 g increase in birthweight was associated with a two point decrease in maternal anxiety in another study [ 29 ]. Birthweight ≤ 1500g was not a significant factor among fathers [ 59 ]. During NNU, BW was not significantly /associated with anxiety in four studies [ 62 , 70 , 73 , 77 ]. No statistically significant difference was found between BW and state anxiety mean scores [ 63 ]. Prematurity (an aggregate of infant BW and age) was not correlated with anxiety scores during NNU [ 70 ]. Apgar scores [ 62 , 73 , 77 ] and infant’s sex [ 63 , 77 , 79 ] were not significantly associated with anxiety. A cumulative neonatal risk factor, based on BW, GA and Apgar scores, was associated with a significant increase in anxiety scores in one study [ 78 ].
4) Infant health and care factors (19 factors: clinicians’ perception of infant’s health, mother-infant attachment and bonding, number of NNU visits, feeding, mothers’ participation in baby care, maternal question asking, interaction with health care professionals, mothers understanding of explanations, length of hospitalisation, brain injury, ventilation, number of days on a ventilator, oxygen treatment, antibiotic treatment, severe neonatal morbidity, development, NNU admission reasons,, NNU room, place discharged/transferred to).
Seven studies [ 27 , 45 , 49 , 61 , 67 , 70 , 76 ] examined the association between clinicians’ perception of infant’s health and parental anxiety. Clinicians’ perception of infant health was measured using varied scales, the clinical risk index for babies (CRIB) score in [ 61 ] and it was a significant risk factor for elevated maternal state anxiety. Similarly, health professional rating of the severity of the infant’s illness assessed via Neurobiologic Risk Score (NBRS) in [ 27 ] was significantly correlated with maternal state anxiety at three months after birth. The influence of infant health status on parental anxiety was apparent during NNU stay in three studies [ 45 , 49 , 70 ]. Presence of an infant health problem was a predictor only at first assessment during NNU [ 45 ]. Whereas infant perinatal risk status using Perinatal Risk Inventory (PERI) correlated significantly with state anxiety during NNU assessment in [ 49 ], and infant illness severity was significantly correlated with anxiety during NNU stay [ 70 ]. Infant health determined using the neonatal risk categorisations by [ 80 ] was not associated with anxiety one week after birth [ 67 ]. Severity of the infant’s condition was not associated with elevated anxiety during NICU stay at two weeks after birth [ 76 ]. Maternal-infant attachment/contact and bonding (physical and verbal) while in NNU was negatively correlated with anxiety symptoms in [ 57 ], but no significant association was found in Lotterman et.al., nor was the number of NNU visits per week, at assessment six months later [ 45 ]. Infant feeding, tube or breast was not significantly associated with more anxiety symptoms in [ 77 ]. Mothers’ participation in infant care while in NNU was reported on in two studies [ 45 , 60 ]. The participation of mothers in many aspects of baby care resulted in reducing state and trait anxiety scores only in [ 60 ]. In [ 45 ] mothers seeking information and asking technical questions e.g. about the equipment and questions related to baby care, and having a positive relationship with healthcare professionals reduced anxiety scores at NNU but the effect was not significant at six months assessment. Whereas, mothers’ receiving explanations from NNU healthcare providers about treatment procedures and infant’s care and being able to understand were perceived as a calming anxiety factor.
Infant length of stay was reported in six studies [ 45 , 59 , 61 , 69 , 70 , 77 ]. A longer hospital stay was correlated with state and trait anxiety scores in one study [ 61 ]. No correlation was found in the remaining studies. Severity of infant brain injury was not correlated with anxiety scores [ 69 ]. One study found that mothers’ to infants who required ventilation had significantly higher anxiety scores [ 79 ]. However the number of days on a ventilator was not correlated significantly with anxiety in another [ 69 ]. Both oxygen treatment and antibiotic treatment were associated with higher anxiety scores in [ 79 ], but severe neonatal morbidity was not associated with higher state or trait anxiety scores at NNU discharge in another study [ 56 ]. Infant development score using a Generalised Developmental Quotient (GQ) [ 81 ] at one year was not correlated with state or trait anxiety in one study [ 49 ].
The reasons for NNU admission, whether it was surgical, medical or for observation, was not associated with more anxiety symptoms at one month post-birth [ 77 ]. Type of neonatal room, whether single or multiple, was not associated with more trait anxiety symptoms [ 56 ]. Place discharged to, home or transfer to another hospital, was not a significant risk factor for increased state anxiety symptoms [ 56 ], whereas being in hospital rather than discharged home was significantly associated with higher anxiety scores [ 79 ].
5) Parental history of mental health problems and trauma factors (Six factors: history of mental condition, history of depression, history of mental health condition any family member, stressful life events, panic and trauma, anxious arousal symptoms).
Three studies [ 45 , 59 , 69 ] reported on the association between parental history of mental health conditions, eg. depression, anxiety or bipolar disorders and developing anxiety, none reported any significant association. Two studies [ 64 , 70 ] looked at the impact of a previous history of depression and both reported a significant correlation with anxiety scores during NNU. A history of mental health problems of any family member and anxiety scores was reported on in [ 59 ] and no significant association with anxiety was found. Stressful life events were not correlated with anxiety scores at NNU discharge in [ 69 ], however, panic and trauma symptoms were significantly correlated with anxiety [ 70 ]. Similarly anxious arousal, a composite variable for panic, was significantly correlated with anxiety [ 70 ].
6) Parental postnatal mental health factors (Three factors: postpartum depression, posttraumatic stress symptoms (PTS), persistent anxiety)
Postpartum depression was reported in eight studies [ 27 , 28 , 31 , 47 , 62 , 70 , 73 , 79 ] all of which found a significant association with anxiety. Postpartum depressive symptoms after birth significantly increased the odds of developing anxiety prior to discharge [ 28 ]. Also, depressive symptoms correlated significantly with state anxiety scores during NNU [ 31 , 62 ], prior to NNU discharge, at two to three weeks after birth [ 79 ], and at three months after birth [ 27 ]. Anxiety symptoms and postpartum depression were significantly correlated during NNU stay [ 70 , 73 ]. Two studies looked at PTS and found a significant correlation between postpartum depression and state anxiety/anxiety [ 27 , 47 ]. Early anxiety symptoms during NNU were not a predictor for anxiety six months later [ 45 ].
7) Parent stress, coping and support factors (Ten factors: Infant’s appearance of stress, stressful sights and sounds, parental role alterations, staff behaviour and communication, PSS scores, coping style, optimism, parents’ resilience, guilt feeling, social support).
Parental stress was measured by Parental Stressor Scale: NICU (PSS: NICU) [ 54 ] in four studies [ 27 , 31 , 59 , 69 ], one further study [ 59 ] reported on PSS four subscales. Infant’s appearance and behaviour stress subscale was reported on in two studies [ 31 , 59 ] and it was found to be a significant stressor for state anxiety in both : In [ 59 ] after birth and at 2–3 weeks afterwards, and in [ 31 ] during NNU assessment. Stressful sights and sounds in NNU were associated with state anxiety only at first assessment after birth in [ 59 ]. Parental role alterations stress (e.g. not being able to feed the infant) in the NNU was a significant factor of more state anxiety symptoms after birth and two to three weeks afterwards in [ 59 ] and during NNU [ 31 ]. In contrast, no correlation was found in [ 69 ]. Stress related to staff-behaviour and communication was not correlated with fathers’ anxiety scores [ 59 ]. Total PSS score measuring overall parental stress was directly correlated with state anxiety at three months after birth in [ 27 ]. Furthermore, elevated PSS scores was associated with higher state anxiety scores in [ 59 ].
The relationship between maternal coping strategies and anxiety level was examined in one study [ 45 ]. Forward coping style was associated with lower anxiety scores during NNU [ 45 ]. There was no significant association between maternal optimism about the infant’s recovery and anxiety scores at six months [ 45 ]. Parents’ resilience was not a risk factor for anxiety during NICU stay at two weeks post birth [ 76 ]. Mothers’ feeling of guilt scores, based on scores for fault, responsibility, punishment, and feelings of helplessness, was significantly correlated with state anxiety scores at two to three weeks after birth [ 79 ].
Fathers’ perception of social support and satisfaction with social support were significantly associated with reduced state anxiety scores soon after birth, but not at a later assessment two to three weeks afterwards [ 59 ]. Similarly, maternal satisfaction with social support was not correlated with anxiety scores at NNU discharge [ 69 ]. How parents perceived social support was not an independent anxiety risk factor during the first two weeks of NNU stay [ 76 ].
8) Other factors (Three factors: bereavement, grief and suffering, maternal physical health)
Two studies [ 58 , 71 ] included parents who experienced bereavement. All parents were bereaved in [ 58 ] and in [ 71 ] bereaved parents were compared to non-bereaved parents. There was a significant correlation between bereavement and anxiety scores among mothers but not fathers [ 58 ]. Bereaved families showed more anxiety symptoms than non-bereaved families even at seven years corrected age [ 71 ], yet no difference was found regarding clinically diagnosed anxiety between the two groups.
The grief/suffering scores at two to six years after the loss of the baby were not significantly correlated with anxiety [ 58 ]. Maternal physical health such as fatigue and shoulder pain were significantly correlated with state anxiety at two to three weeks after birth in [ 79 ].
This review is the first to systematically synthesise factors associated with PTS and anxiety symptoms among parents of infants admitted to NNU. There was significant methodological variability across the 49 included studies, involving 8,447 parents. This was due to differences in study design, inclusion criteria, timing of assessment, measuring tools and cut-off values used. There was also vast variations in defining and reporting on similar factors across the included studies. Therefore, the findings were synthesised narratively.
Although the majority of the identified factors were based on one or two small studies, several factors emerged from multiple studies that could allow healthcare professionals to determine which of these parents require more attention, early screening, referral and intervention before developing PTS and anxiety. Healthcare professionals should target those parents with previous diagnoses of mental health problems before pregnancy and parents who develop any mental health conditions during antenatal and postnatal periods. As seen in the general perinatal population, anxiety, depression and PTS are all highly comorbid conditions among parents of NNU infants [ 82 , 83 , 84 , 85 ].
Factors specific to this population associated with PTS or anxiety included preterm birth (≤ 33 weeks), having an extremely low birthweight (< 1000 g) infant and stressors in the NNU environment, in particular the infants’ appearance and behaviour. Unexpectedly, a number of factors specific to this group of parents showed no association with PTS or anxiety, such as reasons for NNU admission, severe neonatal morbidity, ventilation duration and number of NNU visits, although these results should be interpreted with caution because each of the findings were based on a single study.
A factor consistently found to be associated with PTS was the parents’ own perception of the severity of the infant’s illness. Also when staff did not convey information clearly, it caused emotional stress to the parents and left them feeling powerless and excluded [ 86 ]. In addition to good communication, active parent involvement in baby’s care while in NNU is a protective factor found in this review to reduce anxiety, as parents felt more comfortable and prepared to care for their baby after discharge [ 87 ] thus enhancing the long term positive impacts for the whole family [ 88 ]. Other studies have found fewer medical interventions to the infant and better infant development was seen after parents making physical contact with their infant while in NNU [ 89 ]. Also participation of parents in baby’s care during NICU, as part of a family centred intervention, was associated with a positive impact on infant’s clinical outcomes and a shorter NNU stay as reported in [ 90 ]. Overall, our findings highlight that protective factors around the care provided include communicating well with parents, asking about their perception of how ill their infant is and involving them in providing care to their infants.
Another protective factor for both PTS and anxiety was positive coping mechanisms used by parents after unexpected NNU admission. Encouraging parents to utilise positive coping or adapt their coping styles, such as by taking ‘time out’ or ‘debriefing’ when things go wrong, could be effective in improving their state of mental health and well-being [ 86 , 87 ]. Parents’ degree of greater perceived social support and having a functioning social support setup also emerged as a protective factor for PTS therefore having wider targeted family psychological support and peer to peer support networks could have a positive impact on parents’ mental health [ 86 ]. Early engagement of peer-to-peer support during NNU stay and beyond discharge has also been found to be effective in improving stress, anxiety and depression symptoms [ 91 , 92 ].
Implications for practice and research
As with the general perinatal population a history of mental health problems and having co-morbid mental health conditions are factors associated with both anxiety and PTS in parents of babies admitted to NNU. Therefore, early screening of all parents for mental health problems is the best way to provide much needed information on which parents may need psychological support. As with the general perinatal population, increased awareness amongst healthcare professionals of the influence of history of mental health and co-morbid mental health problems is important in understanding the mental health needs of parents. Parent’s perception of infant illness is a distinctive factor for this group. Therefore clear communication, enquiring into the parents’ perception of their infant’s illness, and early participation of parents in the care of their babies may also ease symptoms of anxiety and PTS.
Bereaved parents are an important subgroup of NNU parents on which there were little data, therefore exploring the needs of these parents while in NNU and their long term comprehensive psychosocial support needs after the loss of the infant is crucial. Another major gap in the literature is the mental health of the fathers and non-traditional family models such as a single parent and same sex families of infants admitted to NNU. Future research should ensure fathers and parents of non-traditional families are included to better understand partner risk factors for PTS and anxiety, and how maternal and partner risk factors interact. Additional research targeting younger parents and those from different ethnic backgrounds is also needed, as are studies in low and middle income settings.
Improving the methodological rigor and standardising approaches to measurement of common mental health problems would add significantly to the current literature. For example, consensus between researchers on the tools and cut-off points for this population is needed. Expanding the scope of routine data collection to include parental risk factors, and linking to existing routine maternity/ primary care data sets would provide population level data to explore parent mental health risk factors more robustly. As many psychosocial risk factors are not routinely collected, a large, more population-based cohort study that additionally includes parents whose babies did not require NNU admission would help better predict the most at risk groups.
Strengths and limitations
The review is a rigorous, comprehensive synthesis of an important research area. We adopted broad, inclusive eligibility criteria and followed a transparent research approach in line with the PRISMA 2020 recommendation. Robust risk of bias assessment and reporting on multivariable analysis, when available, helped reduce the risk of bias in reporting and interpretation of findings. A large number of studies were included in the review, however, despite comprehensive searching and contacting authors, the full texts from 11 studies could not be retrieved. It was not possible to separate out ASD and PTSD in the review as studies collected data over different time periods and often did not differentiate the one month cut-off for ASD. Meta-analysis of data was not feasible as many of the risk factors were examined in one study only, and where more than one study described a risk factor there was considerable methodological heterogeneity in study design, analysis, confounder factors and reporting, combined with clinical heterogeneity, different measures/cut-off points and variation in assessment time. While the data were too heterogeneous to meta-analyse, visually mapping the evidence provides an informative summary of the magnitude of data available for each risk factor.
There is insufficient evidence to support a targeted approach to identifying parents at risk of developing anxiety and PTS when their baby is admitted to NNU. As with the general perinatal population, previous mental health and current co-morbid depression are risk factors for anxiety and PTS. Taking time to communicate well with parents and understand their perceptions of infants’ health may protect parents from experiencing anxiety and PTS symptoms. More research is needed to understand the impact of the NNU environment on parents’ mental health and also the association of low birth weight and a shorter gestational age with anxiety and PTS symptoms. There is some evidence, albeit limited, to suggest that engaging parents early in baby’s care and providing adequate social support may benefit the parents’ mental health. In the absence of evidence to support a targeted approach, routine screening for PTS and anxiety should be offered to all parents, even though, the optimal screening tool and the best administration time are not yet well established for this population.
Availability of data and materials
All data generated during this study are included in this published article and its supplementary information files.
Hawes K, McGowan E, O’Donnell M, Tucker R, Vohr B. Social Emotional Factors Increase Risk of Postpartum Depression in Mothers of Preterm Infants. J Pediatr. 2016;179:61–7.
Article PubMed Google Scholar
Williams KG, Patel KT, Stausmire JM, Bridges C, Mathis MW, Barkin JL. The Neonatal Intensive Care Unit: Environmental Stressors and Supports. Int J Environ Res Public Health. 2018;15(1):60.
Article PubMed PubMed Central Google Scholar
Roque ATF, Lasiuk GC, Radünz V, Hegadoren K. Scoping Review of the Mental Health of Parents of Infants in the NICU. J Obstet Gynecol Neonatal Nurs. 2017;46(4):576–87.
Vigod S, Villegas L, Dennis C-L, Ross L. Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: a systematic review. BJOG: An Int J Obstet Gynaecol. 2010;117(5):540–50.
Article CAS Google Scholar
Malouf R, Harrison S, Burton HAL, Gale C, Stein A, Franck LS, et al. Prevalence of anxiety and post-traumatic stress (PTS) among the parents of babies admitted to neonatal units: A systematic review and meta-analysis. EClinicalMedicine. 2022;43: 101233.
Lakshmanan A, Agni M, Lieu T, Fleegler E, Kipke M, Friedlich PS, et al. The impact of preterm birth <37 weeks on parents and families: a cross-sectional study in the 2 years after discharge from the neonatal intensive care unit. Health Qual Life Outcomes. 2017;15(1):38-.
Qin X, Liu C, Zhu W, Chen Y, Wang Y. Preventing Postpartum Depression in the Early Postpartum Period Using an App-Based Cognitive Behavioral Therapy Program: A Pilot Randomized Controlled Study. Int J Environ Res Public Health. 2022;19(24):16824.
NICE, editor. NICEimpact maternity and neonatal care-Maternity and mental health. https://www.nice.org.uk/about/what-we-do/into-practice/measuring-the-use-of-nice-guidance/impact-of-our-guidance/niceimpact-maternity/ch2-maternity-and-mental-health2023 .
Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J Affect Disord. 2016;191:62–77.
Soto-Balbuena C, Rodríguez MF, Escudero Gomis AI, Ferrer Barriendos FJ, Le HN, Pmb-Huca G. Incidence, prevalence and risk factors related to anxiety symptoms during pregnancy. Psicothema. 2018;30(3):257–63.
PubMed Google Scholar
Giacchino T, Karkia R, Zhang W, Beta J, Ahmed H, Akolekar R. Kielland’s rotational forceps delivery: A comparison of maternal and neonatal outcomes with rotational ventouse or second stage caesarean section deliveries. Eur J Obstet Gynecol Reprod Biol. 2020;254:175–80.
Fischbein RL, Nicholas L, Kingsbury DM, Falletta LM, Baughman KR, VanGeest J. State anxiety in pregnancies affected by obstetric complications: A systematic review. J Affect Disord. 2019;257:214–40.
Furuta M, Sandall J, Cooper D, Bick D. Predictors of birth-related post-traumatic stress symptoms: secondary analysis of a cohort study. Arch Womens Ment Health. 2016;19(6):987–99.
Martinez-Vázquez S, Rodríguez-Almagro J, Hernández-Martínez A, Martínez-Galiano JM. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. Journal of Personalized Medicine. 2021;11(5):338.
Chan SJ, Ein-Dor T, Mayopoulos PA, Mesa MM, Sunda RM, McCarthy BF, et al. Risk factors for developing posttraumatic stress disorder following childbirth. Psychiatry Res. 2020;290: 113090.
NHS & DH. NHS & DH. DEPARTMENT OF HEALTH. 2009. Toolkit for High Quality Neonatal Services. http://www.londonneonatalnetwork.org.uk/wp-content/uploads/2015/09/Toolkit-2009.pdf . Accessed June 2022 2009.
Stark AR. Levels of neonatal care. Pediatrics. 2004;114(5):1341–7.
American Psychiatric Association. Anxiety disorders. In Diagnostic and statistical manual of mental disorders. 5th. ed2013.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Covidence systematic review software. Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org .
Wells G, Shea B OCD, Peterson J, Welch V, Losos M, Tugwell P The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2013, http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp ,. 2013.
Anchan J, Jones S, Aden J, Ditch S, Fagiana A, Blauvelt D, et al. A different kind of battle: the effects of NICU admission on military parent mental health. J Perinatol. 2021;41(8):2038–47.
Brunson E, Thierry A, Ligier F, Vulliez-Coady L, Novo A, Rolland AC, et al. Prevalences and predictive factors of maternal trauma through 18 months after premature birth: A longitudinal, observational and descriptive study. PLoS ONE. 2021;16(2):e0246758.
Article CAS PubMed PubMed Central Google Scholar
Chang HP, Chen JY, Huang YH, Yeh CJ, Huang JY, Su PH, et al. Factors Associated with Post-Traumatic Symptoms in Mothers of Preterm Infants. Arch Psychiatr Nurs. 2016;30(1):96–101.
Clark OE, Fortney CA, Dunnells ZDO, Gerhardt CA, Baughcum AE. Parent Perceptions of Infant Symptoms and Suffering and Associations With Distress Among Bereaved Parents in the NICU. J Pain and Symptom Manage. 2021;62(3):e20–7.
Article Google Scholar
Eutrope J, Thierry A, Lempp F, Aupetit L, Saad S, Dodane C, et al. Emotional reactions of mothers facing premature births: Study of 100 mother-infant dyads 32 gestational weeks. PLoS ONE. 2014;9(8):e104093.
Garfield L, Holditch-Davis D, Carter CS, McFarlin BL, Schwertz D, Seng JS, et al. Risk factors for postpartum depressive symptoms in low-income women with very low-birth-weight infants. Adv Neonatal Care. 2015;15(1):E3–8.
Greene MM, Rossman B, Patra K, Kratovil AL, Janes JE, Meier PP. Depression, anxiety, and perinatal-specific posttraumatic distress in mothers of very low birth weight infants in the neonatal intensive care unit. J Dev Behav Pediatr. 2015;36(5):362–70.
Greene MM, Schoeny M, Rossman B, Patra K, Meier PP, Patel AL. Infant, Maternal, and Neighborhood Predictors of Maternal Psychological Distress at Birth and Over Very Low Birth Weight Infants’ First Year of Life. J Dev Behav Pediatr. 2019;40(8):613–21.
Hawthorne DM, Youngblut JM, Brooten D. Parent Spirituality, Grief, and Mental Health at 1 and 3 Months After Their Infant’s/Child’s Death in an Intensive Care Unit. J Pediatr Nurs. 2016;31(1):73–80.
Holditch-Davis D, Miles MS, Weaver MA, Black B, Beeber L, Thoyre S, et al. Patterns of distress in African-American mothers of preterm infants. J Dev Behav Pediatr. 2009;30(3):193–205.
Jubinville J, Newburn-Cook C, Hegadoren K, Lacaze-Masmonteil T. Symptoms of acute stress disorder in mothers of premature infants. Adv Neonatal Care. 2012;12(4):246–53.
Kim WJ, Lee E, Kim KR, Namkoong K, Park ES, Rha DW. Progress of PTSD symptoms following birth: A prospective study in mothers of high-risk infants. J Perinatol. 2015;35(8):575–9.
Article CAS PubMed Google Scholar
Lefkowitz DS, Baxt C, Evans JR. Prevalence and correlates of posttraumatic stress and postpartum depression in parents of infants in the Neonatal Intensive Care Unit (NICU). J Clin Psychol Med Settings. 2010;17(3):230–7.
Malin KJ, Johnson TS, McAndrew S, Westerdahl J, Leuthner J, Lagatta J. Infant illness severity and perinatal post-traumatic stress disorder after discharge from the neonatal intensive care unit. Early Hum Dev. 2020;140:104930.
Misund AR, Nerdrum P, Braten S, Pripp AH, Diseth TH. Long-term risk of mental health problems in women experiencing preterm birth: A longitudinal study of 29 mothers. Ann Gen Psychiatry. 2013;12(1):33.
Misund AR, Nerdrum P, Diseth TH. Mental health in women experiencing preterm birth. BMC Pregnancy Childbirth. 2014;14(1):263.
Naeem AT, Shariat M, Zarkesh MR, Abedinia N, Bakhsh ST, Nayeri F. The incidence and risk factors associated with posttraumatic stress disorders among parents of NICU hospitalized preterm neonates. Iranian J Neonatol. 2019;10(4):76–82.
Google Scholar
Pace CC, Anderson PJ, Lee KJ, Spittle AJ, Treyvaud K. Posttraumatic Stress Symptoms in Mothers and Fathers of Very Preterm Infants Over the First 2 Years. J Dev Behav Pediatr. 2020;41(8):612–8.
Rodriguez DC, Ceriani-Cernadas JM, Abarca P, Edwards E, Barrueco L, Lesta P, et al. Chronic post-traumatic stress in mothers of very low birth weight preterm infants born before 32 weeks of gestation. Arch Argent Pediatr. 2020;118(5):306–12.
Sharp M, Huber N, Ward LG, Dolbier C. NICU-Specific Stress following Traumatic Childbirth and Its Relationship with Posttraumatic Stress. J Perinat Neonat Nurs. 2021;35(1):57–67.
Shaw RJ, Bernard RS, Deblois T, Ikuta LM, Ginzburg K, Koopman C. The relationship between acute stress disorder and posttraumatic stress disorder in the neonatal intensive care unit. Psychosomatics. 2009;50(2):131–7.
Vinall J, Noel M, Disher T, Caddell K, Campbell-Yeo M. Memories of infant pain in the neonatal intensive care unit influence posttraumatic stress symptoms in mothers of infants born preterm. Clin J Pain. 2018;34(10):936–43.
Williams AB, Hendricks-Munoz KD, Parlier-Ahmad AB, Griffin S, Wallace R, Perrin PB, et al. Posttraumatic stress in NICU mothers: modeling the roles of childhood trauma and infant health. J Perinat. 2021;41(8):2009–18.
Lotterman JH. Factors impacting psychological and health outcomes in mothers and infants following NICU hospitalization of the infant. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2018;79(1-B E). https://doi.org/10.7916/D83R1591 .
Malin KJ, Johnson TS, Brown RL, Leuthner J, Malnory M, White-Traut R, et al. Uncertainty and perinatal post-traumatic stress disorder in the neonatal intensive care unit. Res Nurs Health. 2022;45(6):717–32.
Moreyra A, Dowtin LL, Ocampo M, Perez E, Borkovi TC, Wharton E, et al. Implementing a standardized screening protocol for parental depression, anxiety, and PTSD symptoms in the Neonatal Intensive Care Unit. Early Hum Dev. 2021;154: 105279.
Salomè S, Mansi G, Lambiase CV, Barone M, Piro V, Pesce M, et al. Impact of psychological distress and psychophysical wellbeing on posttraumatic symptoms in parents of preterm infants after NICU discharge. Ital J Pediatr. 2022;48(1):13.
Pisoni C, Spairani S, Fauci F, Ariaudo G, Tzialla C, Tinelli C, et al. Effect of maternal psychopathology on neurodevelopmental outcome and quality of the dyadic relationship in preterm infants: an explorative study. J Matern Fetal Neonatal Med. 2020;33(1):103–12.
Kim DW, Kim HG, Kim JH, Park K, Kim HK, Jang JS, et al. Randomized phase III trial of irinotecan plus cisplatin versus etoposide plus cisplatin in chemotherapy-naive Korean patients with extensive-disease small cell lung cancer. Cancer Res Treat. 2019;51(1):119–27.
Scheiner AP, Sexton ME. Prediction of developmental outcome using a perinatal risk inventory. Pediatrics. 1991;88(6):1135–43.
Brazy JE, Goldstein RF, Oehler JM, Gustafson KE, Thompson RJ Jr. Nursery neurobiologic risk score: levels of risk and relationships with nonmedical factors. J Dev Behav Pediatr. 1993;14(6):375–80.
Crittenden PM. CARE-Index. Coding Manual. 1979–2004.
Miles MS, Funk SG, Carlson J. Parental Stressor Scale: neonatal intensive care unit. Nurs Res. 1993;42(3):148–52.
Bonanno GA, Pat-Horenczyk R, Noll J. Coping flexibility and trauma: The Perceived Ability to Cope With Trauma (PACT) scale. Psychol Trauma Theory Res Pract Policy. 2011;3(2):117–29.
Blanc J, Rességuier N, Lorthe E, Goffinet F, Sentilhes L, Auquier P, et al. Association between extremely preterm caesarean delivery and maternal depressive and anxious symptoms: a national population-based cohort study. Int J Obstet Gynaecol. 2021;128(3):594–602.
Bonacquisti A, Geller PA, Patterson CA. Maternal depression, anxiety, stress, and maternal-infant attachment in the neonatal intensive care unit. J Reprod Infant Psychol. 2020;38(3):297–310.
Buchi S, Morgeli H, Schnyder U, Jenewein J, Hepp U, Jina E, et al. Grief and post-traumatic growth in parents 2–6 years after the death of their extremely premature baby. Psychother Psychosom. 2007;76(2):106–14.
Cajiao-Nieto J, Torres-Gimenez A, Merelles-Tormo A, Botet-Mussons F. Paternal symptoms of anxiety and depression in the first month after childbirth: A comparison between fathers of full term and preterm infants. J Affect Disord. 2021;282:517–26.
Cakmak E, Karacam Z. The correlation between mothers’ participation in infant care in the NICU and their anxiety and problem-solving skill levels in caregiving. Journal of Maternal-Fetal and Neonatal Medicine. 2018;31(1):21–31.
Carvalho AE, Martinez FE, Linhares MB. Maternal anxiety and depression and development of prematurely born infants in the first year of life. Spanish Journal of Psychology. 2008;11(2):600–8.
Dantas MMrC, de Araújo PCB, Santos LcMdO, Pires NA, Maia ElMC. Symptoms of anxiety and depression in mothers of hospitalized premature infants. J Nurs UFPE /Revista de Enfermagem UFPE. 2012;6(2):279–87.
Damanabad ZH, Valizadeh L, Arani MM, Hosseini M, Jafarabadi MA, Mansourian M, et al. Evaluation of Maternal Anxiety in Mothers of Infants Admitted to the Neonatal Intensive Care Unit. Int J Pediatr-Mashhad. 2019;7(10):10215–24.
Das A, Gordon-Ocejo G, Kumar M, Kumar N, Needlman R. Association of the previous history of maternal depression with post-partum depression, anxiety, and stress in the neonatal intensive care unit. J Matern-Fetal Neonat Med. 2021;34(11):1741–6.
Feeley N, Gottlieb L, Zelkowitz P. Mothers and fathers of very low-birthweight infants: Similarities and differences in the first year after birth. J Obstet, Gynecol Neonatal Nurs. 2007;36(6):558–67.
Fontoura FC, Cardoso M, Rodrigues SE, de Almeida PC, Carvalho LB. Anxiety of mothers of newborns with congenital malformations in the pre- and postnatal periods. Rev Lat Am Enfermagem. 2018;26:e3080.
Gennaro S. Postpartal anxiety and depression in mothers of term and preterm infants. Nurs Res. 1988;37(2):82–5.
Mulder RT, Carter JD, Frampton CMA, Darlow BA. Good two-year outcome for parents whose infants were admitted to a neonatal intensive care unit. [References] Psychosomatics. 2014;55(6):613–20.
Rogers CE, Kidokoro H, Wallendorf M, Inder TE. Identifying mothers of very preterm infants at-risk for postpartum depression and anxiety before discharge. J Perinatol. 2013;33(3):171–6.
Segre LS, McCabe JE, Chuffo-Siewert R, O’Hara MW. Depression and anxiety symptoms in mothers of newborns hospitalized on the neonatal intensive care unit. Nurs Res. 2014;63(5):320–32.
Treyvaud K, Aldana AC, Scratch SE, Ure AM, Pace CC, Doyle LW, et al. The influence of multiple birth and bereavement on maternal and family outcomes 2 and 7years after very preterm birth. Early Human Dev. 2016;100:1–5.
Zanardo V, Freato F, Cereda C. Level of anxiety in parents of high-risk premature twins. Acta Genet Med Gemellol. 1998;47(1):13–8.
CAS PubMed Google Scholar
Khemakhem R, Bourgou S, Selmi I, Azzabi O, Belhadj A, Siala N. Preterm birth, mother psychological state and mother- infant bonding. Tunis Med. 2020;98(12):992–7.
Kong L-P, Cui Y, Qiu Y-F, Han S-P, Yu Z-B, Guo X-R. Anxiety and depression in parents of sick neonates: A hospital-based study. [References]J Clin Nurs. 2013;22(7–8):1163–72.
Dickinson C, Vangaveti V, Browne A. Psychological impact of neonatal intensive care unit admissions on parents: A regional perspective. Aust J Rural Health. 2022;30(3):373–84.
Okito O, Yui Y, Wallace L, Knapp K, Streisand R, Tully C, et al. Parental resilience and psychological distress in the neonatal intensive care unit. J Perinatol. 2022;42(11):1504–11.
Shivhare AS R., Choudhary P. P., Alok R. Stressful Experiences of Mothers of Neonates or Premature Infants in a Neonatal Intensive Care Unit. Int J Pharm Clin Res. 2022;14(7):117–26.
Vizcarrondo-Oppenheimer M, García-Coll C, Martínez-González J, Reyes-Bou Z, García-Fragoso L, Sanchez D, et al. Cumulative risk factors and mental health of mothers of infants admitted to the neonatal intensive care unit. J Matern Fetal Neonatal Med. 2021;34(4):660–2.
Park J, Bang KS. The physical and emotional health of South Korean mothers of preterm infants in the early postpartum period: a descriptive correlational study. Child Health Nurs Res. 2022;28(2):103–11.
Blumberg NL. Effects of neonatal risk, maternal attitude, and cognitive style on early postpartum adjustment. J Abnorm Psychol. 1980;89:139–50.
Griffiths R, Huntley M. The Griffiths Mental Development Scales: From Birth to Two Years : Manual: ARICD; 1996.
Molgora S, Fenaroli V, Prino LE, Rollè L, Sechi C, Trovato A, et al. Fear of childbirth in primiparous Italian pregnant women: The role of anxiety, depression, and couple adjustment. Women and Birth. 2018;31(2):117–23.
Yonkers KA, Smith MV, Forray A, Epperson CN, Costello D, Lin H, et al. Pregnant women with posttraumatic stress disorder and risk of preterm birth. JAMA Psychiat. 2014;71(8):897–904.
Cena L, Gigantesco A, Mirabella F, Palumbo G, Camoni L, Trainini A, et al. Prevalence of comorbid anxiety and depressive symptomatology in the third trimester of pregnancy: Analysing its association with sociodemographic, obstetric, and mental health features. J Affect Disord. 2021;295:1398–406.
González-Mesa E, Kabukcuoglu K, Blasco M, Körükcü O, Ibrahim N, González-Cazorla A, et al. Comorbid anxiety and depression (CAD) at early stages of the pregnancy. A multicultural cross-sectional study. J Affect Disord. 2020;270:85–9.
Franck LS, McNulty A, Alderdice F. The Perinatal-Neonatal Care Journey for Parents of Preterm Infants: What Is Working and What Can Be Improved. J Perinat Neonatal Nurs. 2017;31(3):244–55.
Adama EA, Adua E, Bayes S, Mörelius E. Support needs of parents in neonatal intensive care unit: An integrative review. J Clin Nurs. 2022;31(5–6):532–47.
Liu T-T, Lei M-J, Li Y-F, Liu Y-Q, Meng L-N, Jin C-D. Effects of parental involvement in infant care in neonatal intensive care units: a meta-analysis. Frontiers of Nursing. 2018;5(3):207–15.
Pineda R, Bender J, Hall B, Shabosky L, Annecca A, Smith J. Parent participation in the neonatal intensive care unit: Predictors and relationships to neurobehavior and developmental outcomes. Early Hum Dev. 2018;117:32–8.
Zhang R, Huang RW, Gao XR, Peng XM, Zhu LH, Rangasamy R, et al. Involvement of Parents in the Care of Preterm Infants: A Pilot Study Evaluating a Family-Centered Care Intervention in a Chinese Neonatal ICU. Pediatr Crit Care Med. 2018;19(8):741–7.
Okereafor A, Umeh J, Burrows J, Anyaebosim C. 1554 Walking in their shoes: supporting the unique journeys of NICU parents. Arch Dis Child. 2021;106(Suppl 1):A412–3.
Fratantoni K, Soghier L, Kritikos K, Jacangelo J, Herrera N, Tuchman L, et al. Giving parents support: a randomized trial of peer support for parents after NICU discharge. J Perinatol. 2022;42(6):730–7.
Download references
Acknowledgements
We would like to thank the information specialist Nia Roberts at the Knowledge centre, Oxford University for her support in developing the search strategy and searching the literature.
This research is funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme, conducted through the Policy Research Unit in Maternal and Neonatal Health and Care, PR-PRU-1217–21202. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Author information
Authors and affiliations.
NIHR Policy Research Unit in Maternal and Neonatal Health and Care National Perinatal Epidemiology Unit Nuffield Department of Population Health, University of Oxford Old Road Campus Headington, Oxford, OX3 7LF, UK
Reem Malouf, Sian Harrison, Victoria Pilkington & Fiona Alderdice
Department of Medical Statistics, London School of Hygiene and Tropical Medicine, London, UK
Charles Opondo
School of Public Health, Faculty of Medicine, Neonatal Medicine, Imperial College London, Chelsea and Westminster Campus, 369 Fulham Road, London, SW10 9NH, UK
Department of Psychiatry, Medical Sciences Division, University of Oxford, Oxford, UK
Medical Research Council/Wits University Rural Public Health and Health Transitions Research Unit (Agincourt), School of Public Health, Faculty of Health Sciences, University of the Witwatersrand Honorary Professor, African Health Research Institute, Johannesburg, KwaZulu Natal, South Africa
African Health Research Institute, Durban, KwaZulu-Natal, South Africa
Department of Family Health Care Nursing, School of Nursing, University of California San Francisco, 2 Koret Way, San Francisco, CA, 94143, USA
Linda S. Franck
School of Nursing and Midwifery, Queens University Belfast, Belfast, UK
Fiona Alderdice
You can also search for this author in PubMed Google Scholar
Contributions
R.M., planned the review with S.H. and F.A., screened abstracts and full text and selected studies for inclusion extracted data, drafted the initial manuscript, and reviewed and revised the manuscript.
S.H. planned the review along with R.M. and F.A., screened abstracts and full text and assessed studies for eligibility for inclusion, crossed checked data extraction, draft the initial manuscript along with R.M. and F.A. and reviewed and revised the manuscript.
V.B. screened abstracts and full texts and extracted data from eligible studies and reviewed the manuscript.
C.O. contributed to the review methodology, tabulating the results and revised the manuscript.
C.G., L.F. and A.S. contributed to the design of the review, reviewed the extracted data and revised the manuscript.
FA conceptualised and designed the review, contributed to data screening and data extraction, supervised initial analysis of data, drafted the initial manuscript with R.M. and S.H., and reviewed and revised the all subsequent manuscripts.
All authors contributed to the intellectual aspects of this work, read and approved the submitted draft of the review.
Corresponding author
Correspondence to Fiona Alderdice .
Ethics declarations
Ethics approval and consent to participate.
No ethical approval was required as data were retrieved from already published studies.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., supplementary material 3., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Malouf, R., Harrison, S., Pilkington, V. et al. Factors associated with posttraumatic stress and anxiety among the parents of babies admitted to neonatal care: a systematic review. BMC Pregnancy Childbirth 24 , 352 (2024). https://doi.org/10.1186/s12884-024-06383-5
Download citation
Received : 25 August 2023
Accepted : 01 March 2024
Published : 09 May 2024
DOI : https://doi.org/10.1186/s12884-024-06383-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Posttraumatic stress symptoms
- Posttraumatic stress disorder
- Neonatal units
- Preterm birth
- Systematic review
BMC Pregnancy and Childbirth
ISSN: 1471-2393
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on the Future of Nursing 2020–2030; Flaubert JL, Le Menestrel S, Williams DR, et al., editors. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. Washington (DC): National Academies Press (US); 2021 May 11.

The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity.
- Hardcopy Version at National Academies Press
2 Social Determinants of Health and Health Equity
As a nurse, we have the opportunity to heal the heart, mind, soul and body of our patients, their families and ourselves. They may forget your name, but they will never forget how you made them feel. —Maya Angelou, author, poet, and civil rights activist
The United States spends more money on health care than any other highly industrialized country, yet it has the highest poverty rate, the greatest income inequality, and some of the poorest health outcomes of the developed countries. Although access to health care is important, health is driven by many factors outside of medical care, including the neighborhood where one lives, the kind of job one has, one’s economic status, one’s level of education, and one’s access to such things as healthy foods and reliable transportation. The roots of health inequities are deep and complex. It is critical that today’s and tomorrow’s nurses understand the extent to which health is shaped by conditions beyond medical care and what it will take to help everyone lead a healthier life. This chapter examines the social determinants of health; how COVID-19 has exacerbated inequities in health among low-income communities and people of color that existed pre-pandemic; and the strategies and tactics that can be used to improve health upstream, midstream, and downstream.
Compared with any other country in the Organisation for Economic Co-operation and Development (OECD), the United States spends more money on health care and still has the highest poverty rate measured by the OECD, the greatest income inequality, and some of the poorest health outcomes among developed countries ( Escarce, 2019 ). For a variety of reasons, low-income individuals, people of color (POC), and residents of rural areas in the United States experience a significantly greater burden of disease and lower life expectancy relative to their higher income, White, and urban counterparts, and this gap has been growing over time ( Escarce, 2019 ). The roots of these inequities are deep and complex, and understanding them can help elucidate how nurses who currently serve a highly diverse population play a pivotal role in addressing social determinants of health (SDOH)—the conditions in the environments in which people live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks—to improve health outcomes and reduce health inequities. To further that understanding, this chapter provides background on SDOH and highlights social factors that disproportionately affect some communities more than others; Chapters 4 and 5 , respectively, describe the role of nurses in addressing these inequities in health and health care. This chapter also describes the impact of the COVID-19 pandemic in exacerbating the negative effects of SDOH and health inequities among low-income communities and POC ( Garcia et al., 2020 ; Kantamneni, 2020 ).
- SOCIAL DETERMINANTS OF HEALTH
The growing evidence for inequities in both health and access to health care has brought added scrutiny to SDOH. The term typically refers to “nonmedical factors influencing health, including health-related knowledge, attitudes, beliefs, or behaviors” (such as smoking) ( Bharmal et al., 2015 , p. 2). Examples of SDOH also include education, employment, health systems and services, housing, income and wealth, the physical environment, public safety, the social environment (including structures, institutions, and policies), and transportation ( NASEM, 2019b ).
SDOH have consequences for the economy, national security, business, and future generations ( NASEM, 2017 ). Box 2-1 lists SDOH in five areas defined by the U.S. Department of Health and Human Services (HHS)—economic stability, education, social and community context, health and health care, and neighborhood and built environment.
Social Determinants of Health.
SDOH affect everyone. They include both the positive and negative aspects of the conditions in which people are born, grow, live, work, and age. At their best, SDOH can be protective of good health. Many people, however, exhibit a pattern of social risk factors (the negative aspects of SDOH) that contribute to increased morbidity and mortality ( NASEM, 2019a ).
A concept related to SDOH is social needs —individual-level nonmedical acute resource needs related to SDOH, such as housing, reliable transportation, and a strong support system at home, that must be met for individuals to achieve good health outcomes and for communities to achieve health equity ( NASEM, 2019a ; Nau et al., 2019 ). Social needs are a person-centered concept that incorporates each person’s perception of his or her own health-related needs, which therefore vary among individuals ( NASEM, 2019a ). The nursing community has long focused on the social needs of people and communities, and has worked closely with social workers and community health workers to address individuals’ more complex social needs ( Foster et al., 2019 ; Gordon et al., 2020 ). Nurse-designed models of care, discussed throughout this report, often successfully integrate the social needs of individuals and families, as documented in a recent RAND report ( Martsolf et al., 2017 ).
Improving population health (e.g., through measures that improve life expectancy) means improving health for everyone. However, historically disadvantaged groups trail dramatically behind others by many measures of health. Health equity is achieved by addressing the underlying issues that prevent people from being healthy. At the population level, health equity can be achieved by addressing SDOH, while at the individual level, it can be achieved by addressing social needs. Health equity benefits everyone through, for example, economic growth, a healthier environment, and national security. At both the population and individual levels, work to improve health and health equity will require cross-sector collaborations and, where necessary, enabling policies, regulations, and community interventions.
Conceptual Frameworks for the Social Determinants of Health
Several frameworks have been developed to explain the interactive nature of how social factors can contribute to health. These frameworks help health professionals and others understand and address SDOH to reduce health disparities and improve health equity. Two important frameworks—the conceptual SDOH framework developed by the World Health Organization’s (WHO’s) Commission on the Social Determinants of Health and the Social Determinants of Health and Social Needs Model of Castrucci and Auerbach (2019) —are described below to show the relationship between health and social factors and strategies for improving health and well-being, providing context for the report’s focus on the nurse’s role in addressing health and health care equity.
Conceptual Social Determinants of Health Framework of the Commission on the Social Determinants of Health
In 2010, WHO’s Commission on the Social Determinants of Health developed a widely used conceptual framework designed to explain the complex relationships between social determinants and health (see Figure 2-1 ). This framework divides SDOH into two categories: structural determinants , defined as SDOH inequities, such as socioeconomic and political context, social class, gender, and ethnicity; and intermediary determinants , defined as such SDOH as material circumstances, psychosocial circumstances, and behavioral and biological factors.
Conceptual framework of the Commission on the Social Determinants of Health. SOURCE: Adapted from Solar and Irwin, 2010.
The WHO model shows how inequities created by policies and structures (structural determinants) underlie community resources and circumstances (intermediary determinants). In this model, social, economic, and political mechanisms contribute to socioeconomic position, characterized by income, education, occupation, gender, race/ethnicity, and other factors that reflect social hierarchy and status. Social standing is related to an individual’s exposures and vulnerability to health conditions. Those structural determinants shape the intermediary determinants—material conditions (e.g., living and working conditions, food security), behaviors and biological factors (e.g., alcohol and tobacco consumption, physical activity), and psychosocial factors (e.g., social support, psychosocial stress) that underlie health. All of these factors impact health, and health can also create a feedback loop back to the structural determinants. For example, poor health or lack of education can impact an individual’s employment opportunities, which in turn constrains income. Low income reduces access to health care and nutritious food and increases hardship (NEJM Catalyst, 2017 ; Solar and Irwin, 2010 ).
The health care system falls in the framework as an intermediary determinant. The impact of the health care system creates another layer of determinants based on differences in access to and quality of care. By improving equitable access to health care and creating multisector solutions to improve health status—such as access to healthy food, transportation, and linkage to other social services as needed—the health care system can address disparities in health ( Solar and Irwin, 2010 ). Furthermore, the health care system provides an opportunity to mediate the indirect consequences of poor health related to deteriorating social status ( Solar and Irwin, 2010 ). Understanding the complex relationship between SDOH and health is essential in order for nurses to address health equity. Accordingly, Chapter 9 highlights the importance of transforming nursing curriculum and continuing education by integrating SDOH to improve health equity.
Social Determinants of Health and Social Needs Model
Throughout this report, the committee uses the Social Determinants of Health and Social Needs Model of Castrucci and Auerbach (2019) to describe the upstream, midstream, and downstream strategies used by nurses to improve individual and population health (see Figure 2-2 ). Upstream factors represent SDOH and affect communities in a broad and inequitable way. Low educational status and opportunity, income disparity, discrimination, and social marginalization are upstream factors that prevent good health outcomes. For example, nurses engage in upstream factors by informing government policies at the local and federal levels. Midstream factors represent social needs, or the individual factors that might affect a person’s health. These are specific nonmedical acute resource needs that lie on the causal path between SDOH and health inequities ( Nau et al., 2019 ). Midstream factors that might prevent a person from achieving optimal health include homelessness, food insecurity, poor access to education, and trauma. Through midstream efforts, nurses focus on preventing disease and meeting social needs—for example, in federally qualified health centers or through public health departments—by screening for such social risk factors as lack of housing and food access and using these data to inform referrals to government and community resources related to the identified social needs. Activities addressing downstream factors include disease treatment and chronic disease management, in which nurses typically engage in settings where health care is delivered, from homes to urgent care clinics to hospitals. Nursing research typically focuses on downstream and midstream factors.
Social Determinants of Health and Social Needs Model. SOURCE: Adapted from Castrucci and Auerbach, 2019.
The majority of nurses work in hospitals and clinics; therefore, most work midstream and downstream providing individual-level interventions to patients. Nonetheless, an understanding of the interrelationships among upstream, midstream, and downstream factors and interventions is necessary to fully comprehend and influence the health of individuals and communities. Moreover, all nurses have the opportunity to work upstream through advocacy for policy changes that promote population health. To engage robustly at all three levels, however, nurses need education, training, and support. The following sections review SDOH and social needs at all three levels of this model, along with their health implications.
- HEALTH IMPLICATIONS OF SOCIAL FACTORS
This section describes social factors into which people are born, that may change as they age, and that have implications for health outcomes. Additionally, it describes factors in the places where people live, including housing and homelessness, food insecurity, environmental factors, and geography/rurality, that also affect health outcomes. Before proceeding, it is important to note that social determinants intersect, with further implications for health (see Box 2-2 ).
Intersectionality.
Race and Racism
Racism, a structural inequity that negatively impacts health and health equity, is “an organized social system in which the dominant racial group, based on an ideology of inferiority, categorizes and ranks people into social groups called ‘races’ and uses its power to devalue, disempower, and differentially allocate valued societal resources and opportunities to groups defined as inferior” ( Williams et al., 2019 , p. 106). Williams and colleagues describe three interrelated forms of racism: structural racism, cultural racism, and discrimination.
Structural racism is racism that is embedded in laws, policies, and institutions and provides advantages to the dominant racial group while oppressing, disadvantaging, or neglecting other racial groups ( Williams et al., 2019 ). Structural racism can be seen in residential segregation, the criminal justice system, the public education system, and immigration policy. Williams and colleagues identify structural racism as the most important way in which racism impacts health. A robust body of evidence on the link between residential segregation and poor health, for example, shows that segregation is associated with outcomes that include low birthweight and preterm birth ( Mehra et al., 2017 ) and lower cancer survival rates ( Landrine et al., 2017 ). However, methodological limitations can make structural racism a challenging topic to study. Researchers have developed some novel measures of the phenomenon, including one that combines indicators of political participation, employment and job status, educational attainment, and judicial treatment ( Lukachko et al., 2014 ). In this study, structural racism is defined by state-level racial disparities across those four domains. Using this measure, the researchers found that Blacks living in states with high levels of structural racism were more likely to experience myocardial infarction relative to Blacks living in states with low levels of structural racism ( Lukachko et al., 2014 ). Another group of researchers developed a measure of state-level structural racism that combines indicators of residential segregation, incarceration rates, educational attainment, economic indicators, and employment status. This study found that higher levels of structural racism were associated with a larger disparity between Black and White victims of fatal police shootings ( Mesic et al., 2018 ).
Structural racism has also contributed to the high incarceration rate in the United States, which exceeds the rates of other countries in which POC make up the majority of the population ( Acker et al., 2019 ). Mass incarceration is a public health crisis that disproportionately impacts Black and Hispanic individuals and their families and communities ( Brinkley-Rubinstein and Cloud, 2020 ; Carson, 2020 ). Individuals who are incarcerated have greater chances of developing chronic health conditions and are exposed to factors, including overcrowding, poor ventilation and sanitation, stress, and solitary confinement, that exacerbate chronic conditions and impact long-term physical and mental health ( Acker et al., 2019 ; Kinner and Young, 2018 ). Evidence shows that following incarceration, mortality rates increase significantly, and individuals also face limited opportunities in employment, housing, and education ( Massoglia and Remster, 2019 ).
The second form of racism, cultural racism , is the “instillation of the ideology of inferiority in the values, language, imagery, symbols, and unstated assumptions of the larger society” ( Williams et al., 2019 , p. 110). Through cultural racism, people absorb and internalize negative stereotypes and beliefs about race, which can both create and support structural and individual racism and create implicit biases ( Williams et al., 2019 ). Implicit bias can in turn lead to unintentional and unconscious discrimination against others. Important in the context of this study is that implicit bias has been shown to be prevalent in health care ( FitzGerald and Hurst, 2017 ; Hall et al., 2015 ) and to result in disparate outcomes among individuals of different races. For example, some research suggests that women of color are less likely than their White counterparts to receive an epidural during childbirth because of providers’ beliefs about the relationship between race and pain tolerance, as well as poor communication in racially discordant provider–patient relationships ( NASEM, 2020 ). Research has also shown that providers perceive Black individuals as less likely than White individuals to adhere to medical advice, a perception that contributes to poor communication and care ( Laws et al., 2014 ; van Ryn and Burke, 2000 ). These experiences of implicit bias, together with a long history of unethical treatment of POC in the health care system, can lead to mistrust and avoidance of the system, thus exacerbating health disparities ( Chaturvedi and Gabriel, 2020 ).
Discrimination is the third—and most researched—form of racism. It occurs when people or institutions treat racial groups differently, with or without intent, and this difference results in inequitable access to opportunities and resources ( Williams et al., 2019 ). Self-reported discrimination, in which the discrimination is perceived by the individual being discriminated against, is often used as an indicator of racism in studies on health care and health outcomes. Self-reported discrimination is believed to impact health by triggering emotional and physiological reactions and by changing an individual’s health behaviors ( Williams et al., 2019 ). It has been associated with poor health in multiple areas, including mental health ( Paradies et al., 2015 ), sleep ( Slopen et al., 2016 ), obesity ( Bernardo et al., 2017 ), hypertension ( Dolezsar et al., 2014 ), and cardiovascular disease ( Lewis et al., 2014 ). In addition to the actual experience of discrimination, just the threat of discrimination—and the associated hypervigilance—can negatively impact health. Discrimination can also be experienced through microaggressions, defined as “brief and commonplace daily verbal, behavioral, or environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults toward people of color” ( Sue et al., 2007 , p. 273). Microaggressions have been correlated with outcomes that include poor mental health ( Cruz et al., 2019 ), poor physical health ( Nadal et al., 2017 ), and sleep disturbance ( Ong et al., 2017 ). Moreover, microaggressions that are experienced within the health care setting may undermine the provider–patient relationship and thus the quality of care ( Cruz et al., 2019 ).
The COVID-19 pandemic has brought the issue of racism as a social determinant into sharp focus, illuminating the mechanisms by which it affects health outcomes. COVID-19 has disproportionately affected Black Americans, Hispanic Americans/Latinos, and American Indians/Alaska Natives (AI/ANs) ( Cuellar et al., 2020 ). Blacks have been more likely to be diagnosed with COVID-19 and more likely to die relative to people of other races. The death rates for COVID-19 among Blacks reported by the Centers for Disease Control and Prevention (CDC) are higher than the rates for non-Hispanic Whites, AI/ANs, Asians, and Hispanics/Latinos ( CDC, 2020a ). Van Dorn and colleagues (2020) also report disproportionately high rates of COVID-19 deaths among African Americans. As of April 2020, when their article was published, three-quarters of all COVID-19 deaths in Milwaukee, Wisconsin, had occurred among African Americans, who also accounted for all but three COVID-related deaths in St. Louis, Missouri. Still, according to CDC, COVID-19 cases were 3.5 times higher among AI/ANs and 2.8 times higher among Hispanics/Latinos than among non-Hispanic Whites ( CDC, 2020b ). Van Dorn and colleagues (2020) point out that AI/AN populations have disproportionately high levels of such underlying conditions as heart disease and diabetes that make them more susceptible to the virus, and the Indian Health Service (IHS), which provides health care for the 2.6 million AI/ANs living on tribal reservations, has only 1,257 hospital beds and 36 intensive care units across the United States, so that many people covered by the IHS are hours away from its nearest facility (van Dorn et al., 2020 ).
Research on the specific mechanisms behind these disparities is ongoing, but there are many potential explanations for the link between race and COVID-19 outcomes. Camara Phyllis Jones, past president of the American Public Health Association, posits that POC are more at risk for four reasons ( Wallis, 2020 ). First, they are more exposed to the risk of infection because they are more likely to live in dense neighborhoods, work in front-line or essential jobs, and be incarcerated or held in immigration facilities (see also van Dorn et al., 2020 ). This set of risk factors is tied to structural racism, including historical and current residential and educational segregation in the United States. Second, POC are less protected from infection because of cultural norms that devalue their lives and their health. Third, POC are more likely to suffer from underlying conditions that put them at risk of poor outcomes once infected. For example, Black Americans are 60 percent more likely to have diabetes and 40 percent more likely to have hypertension relative to their White counterparts ( HHS, 2019 , 2020 ). These conditions, says Jones, are due to the context of their lives—the lack of healthy food choices, more polluted air, and few places to exercise safely. Finally, POC are less likely to have access to quality health care (and thus are more likely to experience unnecessary treatments, inaccurate diagnoses, and medication errors), and more commonly face structural and individual discrimination within the health care system. Yancy (2020) echoes this analysis, noting that social distancing—one of the most effective strategies for reducing transmission of COVID-19—is a privilege that is unavailable to many POC because of where they live and work.
The confluence in 2020 of the COVID-19 pandemic and the Black Lives Matter 1 protests has brought new opportunities for nurses to be involved in dismantling racism. For example, while the American Nurses Association (ANA) issued a position statement in 2018 opposing individual and organizational discrimination (ANA Ethics Advisory Board, 2019 ), its 2020 resolution took an even stronger stand, calling for an end to systemic racism and health inequities and condemning brutality by law enforcement ( ANA, 2020 ). The executive director of National Nurses United, Bonnie Castillo, stated in June 2020 that “it is racism that is the deadly disease,” as reflected in disparities in health, police killings, housing, employment, criminal justice, and other areas ( NNU, 2020 ). Nurses are attending protests to offer aid to injured protestors, despite the threat of tear gas and rubber bullets ( Jividen, 2020 ).
Income and Wealth
Higher income (earnings and other money acquired annually) is associated with a lower likelihood of disease and premature death ( Woolf et al., 2015 ). The relationship of wealth (net worth and assets) to health outcomes shows a similar relationship with disease and premature death. Studies have found longitudinal associations between higher levels of wealth and better health outcomes that include lower mortality, higher life expectancy, slower declines in physical functioning, and decreased risk of smoking and hypertension ( Hajat et al., 2010 ; Kim and Richardson, 2012 ; Zagorsky and Smith, 2016 ). Significant health-related differences exist between the income levels of individuals below 100 percent and above 200 percent of the federal poverty level.
With respect to life expectancy, the expected age at death among 40-year-olds is lowest for individuals with the lowest household income and increases as household income rises ( Escarce, 2019 ). Notably, this is a continuous gradient (see Figure 2-3 ). Between women in the top 1 percent and the bottom 1 percent of income, there is a 10-year difference in life expectancy. This disparity is greater among men, for whom this gap rises to 15 years. These trends have been worsening over time. Since 2000, individuals in all income groups have gained in life expectancy, but the highest earners have had the highest gains, and the gap in life expectancy between the highest and lowest earners is increasing ( Escarce, 2019 ).
Expected age at death among 40-year-old men and women, by household income percentile. SOURCES: Escarce, 2019; reproduced from Chetty et al., 2016.
Income correlates highly as well with risk factors for chronic disease and mental health conditions. Relative to people with higher family income, for example, people with lower family income have higher rates of heart disease, stroke, diabetes, and hypertension and are more likely to have four or more common chronic conditions ( NCHS, 2017 ). People in families whose income is below 200 percent of the federal poverty level are more likely than people in families with higher income to be obese and to smoke cigarettes. Adults who live in poverty are also more likely to have self-reported serious psychological distress—6.4 percent of those making less than $35,000 feel sadness and 3.8 percent feel worthlessness, compared with 1.3 percent and 0.6 percent, respectively, of those making $75,000–$99,999 ( Weissman et al., 2015 ; Woolf et al., 2015 ).
In addition to impacting the safety and quality of neighborhoods and schools, parental income and wealth can affect the resources and support available within families ( Chetty and Hendren, 2018 ). Children in low-income families typically face barriers to educational and social opportunities, which in turn limits their social mobility and good health as adults ( Braveman et al., 2018 ; Killewald et al., 2017 ; Odgers and Adler, 2018 ; Owen and Candipan, 2019 ). As health and socioeconomic disadvantages accumulate over a person’s lifetime, this pattern of inequity, exacerbated by structural barriers, can persist across generations, preventing intergenerational social mobility ( Braveman et al., 2018 ; Chetty et al., 2014 ).
Access to Health Care
Equitable access to health care is needed for “promoting and maintaining health, preventing and managing disease, reducing unnecessary disability and premature death, and achieving health equity” ( ODPHP, 2020b ). Evidence shows that access to primary care prevents illness and death and is associated with positive health outcomes ( Levine et al., 2019 ; Macinko et al., 2007 ; Shi, 2012 ). Access to health care services is therefore an important SDOH, and inequities in multiple factors, such as a lack of health insurance coverage and limited availability of health care providers, limit that access.
Studies have shown that individuals without health insurance are much less likely to receive preventive care and care for major health conditions and chronic diseases ( Cole et al., 2018 ; Seo et al., 2019 ). In a study of nonelderly adult patients, insured versus uninsured individuals were more likely to obtain necessary medical care, see a recommended specialist, see a mental health professional if advised, receive recommended follow-up care after an abnormal pap test, and get necessary prescription medications ( Cole et al., 2018 ). Lack of insurance is also associated with a lower likelihood of receiving treatments recommended by health care providers and longer appointment wait times ( Chou et al., 2018 ; Fernandez-Lazaro et al., 2019 ). In one study, two groups posing as new patients discharged from the emergency department requested follow-up appointments. Those who claimed commercial insurance were more likely than the Medicaid-insured group to receive care within 7 days ( Chou et al., 2018 ).
Wide income and racial/ethnic inequities in insurance coverage therefore have a significant effect on access to health care services, thus influencing health equity. In the United States, African American and Hispanic individuals have a higher risk of being uninsured relative to non-Hispanic Whites ( Artiga et al., 2020 ). Census Bureau data indicate that Hispanics face the greatest barriers to health insurance: between 2017 and 2018, the uninsurance rate increased from 16.2 to 17.8 percent for Hispanics, from 9.3 to 9.7 percent for Blacks, from 6.4 to 6.8 percent for Asians, and from 5.2 to 5.4 percent for non-Hispanic Whites ( Barnett et al., 2019 ). American Indians have high uninsured rates; CDC reports that 28.6 percent of these individuals under age 65 are uninsured ( HHS, 2018 ). It is important to note that uninsured people often delay or forgo care because of its cost and are less likely than those with insurance to have a usual source of care or receive preventive care ( Amin et al., 2019 ), which can lead them to experience serious illness or other health problems. Chapter 4 provides information on nursing’s role in expanding access to health care.
Access to Education
Lower-income families often live in school districts that are resource-poor, and they lack the resources available to upper-income families for making investments in early childhood enrichment activities. Over time, the gap between the rich and poor with respect to receiving higher education has widened. Children born in 1979–1982 were 18 percent more likely to complete college if their parents were in the highest relative to the lowest income quartile. More recently, this percentage has grown to 69.2 percent ( Woolf et al., 2015 ).
Hahn and Truman (2015) report a strong association between educational attainment and both morbidity and mortality. In the United States, adults with lower educational attainment have higher rates of major circulatory diseases; diabetes; liver diseases; and such psychological symptoms as feelings of sadness, hopelessness, and worthlessness (although those with higher levels of educational attainment experience higher rates of prostate cancer and sinusitis). As for life expectancy, in 2017 a White man in the United States with less than a high school education could expect to live 73.5 years, while his counterpart with a graduate degree could expect to live more than 10 years longer. Likewise, a White woman could expect to live 8 years longer if she had a graduate degree than if she had less than a high school degree ( Sasson and Howard, 2019 ).
Housing Instability and Homelessness
Research shows that people need stable housing to be healthy; people with limited resources and unstable housing are exposed to a number of health risks but often cannot move to better neighborhoods ( Woolf et al., 2015 ). Homelessness also is closely linked to poor physical and mental health. Homeless people experience higher rates of such health problems as HIV, alcohol and drug abuse, mental illness, tuberculosis, and other conditions ( Aldridge et al., 2018 ; Mosites et al., 2020 ). Providing stable housing coupled with such services as case management has been shown to improve mental health and health status in both children and parents ( Bovell-Ammon et al., 2020 ).
Researchers have identified four pathways by which housing and health are connected ( Taylor, 2018 ):
- The stability pathway : As noted above, not having stable housing has negative effects on health. Health problems among youth associated with residential instability include increased risk of teen pregnancy, early drug use, and depression ( Taylor, 2018 ).
- The quality and safety pathway : A number of negative environmental factors within homes are correlated with poor health. In-home exposure to lead irreversibly damages the brains and nervous systems of children. Substandard housing conditions, such as water leaks, poor ventilation, poor air quality, dirty carpets, mold, and pest infestation, have been associated with poor health outcomes, most notably asthma ( Taylor, 2018 ).
- The affordability pathway : A lack of affordable housing options can affect families’ ability to meet other essential expenses and create serious financial strain. Low-income families with difficulty paying rent or utilities are less likely to have a usual source of medical care and more likely to postpone needed treatment ( Taylor, 2018 ).
- The neighborhood pathway : Researchers have found that the availability of resources, such as public transportation to one’s job, grocery stores with nutritious foods, and safe spaces to exercise, is correlated with better health outcomes ( Taylor, 2018 ).
Food Insecurity
Food-insecure households are those that lack the resources to purchase adequate food to maintain their health. The U.S. Department of Agriculture (USDA) estimates that in 2018, 11.1 percent of U.S. households were food-insecure at some time during the year ( USDA, 2020 ). Residents of low-resource neighborhoods often have limited access to sources of healthy food, such as supermarkets that sell fresh produce and other healthful food options. They are more likely to live in food deserts, characterized by an overconcentration of fast food outlets, corner stores, and liquor stores and a shortage of options for fresh fruits and vegetables and restaurants that offer healthy choices and menu labeling ( Woolf et al., 2015 ).
Gundersen and Ziliak (2015) reviewed the literature on the effect of food insecurity on health in the United States. They found that the majority of research in this area has focused on children, revealing that food insecurity is associated with birth defects, anemia, lower nutrient intakes, cognitive problems, and aggression and anxiety, as well as higher hospitalization rates, poorer general health, asthma, behavioral problems, depression, suicidal ideation, and poor oral health. The authors also found that food insecurity is more common in households headed by an African American or Hispanic person and households with children ( Gundersen and Ziliak, 2015 ). COVID-19 has exacerbated food insecurity; Feeding America estimates that almost 17 million individuals may have experienced food insecurity during the pandemic ( Balch, 2020 ).
Environment and Climate Change
Environmental conditions affect the health of all individuals and communities. Environmental hazards, such as air pollution, harmful agricultural chemicals, and poor water quality, are more likely to exist in low-income communities and those populated by POC, and those communities tend to be more vulnerable to such hazards. Additionally, while natural disasters, such as floods, hurricanes, tornadoes, fires, winter storms, drought, and earthquakes, pose great threats to life and property and strain emergency and health care services wherever they strike, they affect underresourced populations more severely. These populations are more likely to live in geographic areas that are at high risk of natural disasters, such as flood plains, and to live in housing that is less resilient, such as mobile homes. Moreover, low-income residents have less capacity to move when such risks become evident ( Boustan et al., 2017 ). In addition, the impacts of natural disasters depend not only on the magnitude of the event but also on the exposure and vulnerability of the population, which vary with levels of wealth and education; disability and health status; and gender, age, class, and other social and cultural characteristics ( IPCC, 2012 ). These inequities become even more pronounced if populations are displaced or forced to evacuate ( Supekar, 2019 ). Natural disasters have long-term economic impacts on communities as well. Research shows that as damages from natural disasters increase, so, too, does wealth inequity in the long term, especially in relation to race, education, and homeownership ( Howell and Elliott, 2018 ).
Researchers have increasingly found evidence that global climate change is increasing the magnitude and frequency of such severe events, including droughts, wildfires, and damaging storms ( McNutt, 2019 ). Extreme weather (heat, drought), flooding, air and water pollution, allergens, vector- and waterborne diseases ( Demain, 2018 ; IFRC, 2019 ), fire and its effects on air quality ( Fann et al., 2018 ), and effects on the food supply related to nutrition and migration ( NASEM, 2018 )—all developments exacerbated by climate change—are already affecting human health around the globe. The changing climate will mean new challenges to health and disproportionate stress on some communities.
Geography is associated with barriers to high-quality health care that can impact health outcomes. Rural Americans face numerous health inequities compared with their urban counterparts. More than 46 million Americans, or 15 percent of the U.S. population, live in rural areas ( CDC, 2017 ). Compared with metropolitan areas, rural areas have higher death rates across the five leading causes of death nationally (heart disease, stroke, cancer, unintentional injury, and chronic lower respiratory disease). Among those aged <80 years in 2014, the numbers of potential excess deaths in rural areas for those five leading causes were 25,278 from heart disease, 19,055 from cancer, 12,165 from unintentional injury, 10,676 from chronic lower respiratory disease, and 4,108 from stroke. Death rates for unintentional injuries are 50 percent higher in rural than in metropolitan areas, attributable mainly to motor vehicle crashes and opioid overdoses ( Garcia et al., 2017 ; Moy et al., 2017 ). Rural relative to urban residents have a higher percentage of several risk factors associated with poorer health. For example, obesity prevalence is significantly higher among rural than urban residents (34.2 percent versus 28.7 percent) ( Lundeen et al., 2018 ).
Inequities within rural areas also exist, particularly at the intersection of geography and race and ethnicity. Based on County Health Rankings data for 2015, rural counties in which the majority of the population was non-Hispanic White had higher median household incomes, lower unemployment rates, fewer households with people younger than 18, and better access to healthy food compared with counties where other racial and ethnic groups made up the majority of the population. Not only did counties with majority Black and majority AI/AN residents have significantly greater potential years of life lost before age 75 relative to counties with predominantly White residents, but also those differences were mediated by sociodemographic characteristics, including household income, unemployment rates, and the number of primary care physicians in the county ( Henning-Smith et al., 2019 ).
Shortages of Health Care Providers
Shortages of health care providers significantly affect access to care in rural areas; as of December 2019, approximately 62.9 percent of primary care health professional shortage areas (HPSAs) were located in rural areas ( RHI, 2020 ). According to the Georgetown University Health Policy Institute, less than 11 percent of U.S. physicians practice in rural areas, while 20 percent of the U.S. population lives in these areas ( Georgetown University, n.d. ). Adding to this challenge is the closure of more than 160 rural hospitals since 2005 as the result of a number of factors, including decreasing profits, consolidation of the health care system, high rates of uninsured, and waning rural populations to support hospitals ( Cecil G. Sheps Center for Health Services Research, 2014a , b ). The decline in rural acute care services highlights the increased need for primary care and individual and community-wide education in these areas to help prevent and manage chronic conditions and avoid related health crises that can lead to hospitalization and death ( RHI, 2020 ).
Health Insurance Status
Uninsured rural residents face greater difficulty accessing care compared with their urban counterparts because of the limited supply of rural health care personnel who can provide low-cost or charity health care ( Newkirk and Damico, 2014 ). According to a June 2016 issue brief from HHS, 43.4 percent of uninsured rural residents reported not having a usual source of care ( Avery et al., 2016 ). The brief also states that 26.5 percent of uninsured rural residents had delayed receiving health care in the past year because of cost constraints. The affordability of health insurance is also a barrier for rural residents ( Barker et al., 2018 ).
Transportation and Internet Access
Transportation poses a barrier to accessing appropriate care for all underresourced populations because of the travel time, cost, and time away from work involved. In rural areas, individuals are more likely to have to travel long distances for care, which can be burdensome given the higher rates of rural versus urban poverty. Longer distances can also result in longer wait times for emergency medical services and endanger individuals seeking prompt care for a potentially life-threatening emergency. Moreover, rural areas lack reliable transportation, whereas urban areas often have public transit available as an option for traveling to appointments.
Telehealth can help mitigate the challenges associated with transportation in rural areas; however, adequate broadband access is often limited in these areas. Almost 33 percent of rural individuals lack access to high-speed broadband Internet, defined by the Federal Communications Commission as download speeds of 25 Mbps or higher ( FCC, 2015 ). Without access to broadband Internet, individuals seeking care cannot access video-based telehealth visits. In Michigan, for example, approximately 40 percent of rural residents lack access to high-speed broadband Internet versus just 3 percent of urban residents ( FCC, n.d. ). Thus, the shift to telehealth during COVID-19 may have exacerbated health disparities for millions of individuals living in rural areas.
- THE COVID-19 PANDEMIC AND HEALTH INEQUITIES
The economic impacts of COVID-19 have been wide-reaching in the face of record high unemployment rates ( BLS, 2020 ). The effects of the pandemic on both health and income have been especially severe for low-income individuals and POC. Internationally, rates of job loss have been high among low-income versus high-income people, further impacting their ability to access such essentials as healthy food ( Daly et al., 2020 ; Lopez et al., 2020 ).
The disproportionate effects of COVID-19 on POC were discussed earlier in the chapter. Undocumented immigrants are another population in the United States that has been particularly vulnerable to the effects of the virus. An estimated 7.1 million undocumented immigrants lack health insurance, and the Patient Protection and Affordable Care Act excludes undocumented immigrants from eligibility for coverage. As a result, many undocumented immigrants lack access to primary care and have relied on emergency departments for years ( Page et al., 2020 ). Although immigrant communities tend to be relatively young and healthy, the prevalence of diabetes, a risk factor for COVID-19, is high (22 percent) among Hispanics ( Page et al., 2020 ). The prevalence of diabetes is also high among AI/ANs—14.7 percent for adults ( CDC, 2018 ). Additionally, as in the African American community, a high proportion of undocumented workers are employed in service industries, such as restaurants and hotels, or in the informal economy, which places them at increased risk of infection.
Another important consideration is the inequity inherent in school closures during the pandemic, which has affected children from underresourced families disproportionately. As with telehealth, access to distance learning is unequal for those who lack access to the Internet or the requisite technologies. Moreover, many underresourced communities rely on subsidized meal programs for adequate nutrition and on school nurses for vaccines and other health care services ( Armitage and Nellums, 2020 ). Schools also may provide safeguarding and supervision, and school closures mean that parents considered essential workers may leave children unsupervised at home or forgo employment to stay at home with them ( Armitage and Nellums, 2020 ). Low-income families have fewer resources to expend on their children’s at-home education, meaning that during the pandemic, their children have fallen further behind relative to higher-income classmates who may have easier access to computers and the Internet while they are distance learning.
People in prisons, nursing homes, homeless shelters, and refugee camps constitute other vulnerable populations at higher risk during the pandemic. Many people in certain congregate settings have inadequate access to even basic health care, and many are older and have preexisting conditions, in addition to their close proximity to other people, that have placed them at high risk of infection ( Berger et al., 2020 ). CDC assessed the prevalence of COVID-19 infections in homeless shelters in four U.S. cities during March 27–April 15, 2020, working with local partners to test residents and staff proactively, and found high levels of COVID-19 in both groups. Specifically, they found that 17 percent of residents and 17 percent of staff in Seattle, Washington; 36 percent of residents and 30 percent of staff in Boston, Massachusetts; and 66 percent of residents and 16 percent of staff in San Francisco, California, tested positive for the virus. Clearly, in many congregate care environments both residents and staff have been at high risk for contracting this disease; the latter, many of whom are low-income, are often deemed essential workers.
Emerging morbidity and mortality data further demonstrate that the effects of the pandemic have fallen disproportionately on vulnerable U.S. populations and exacerbate the deeply rooted social, racial, and economic disparities to which these populations are subject. Berger and colleagues (2020) note that underserved communities are distrustful of public health institutions, which have historically mistreated them, and suggest that it is unfair to ask them to act in the public interest by staying home at the expense of supporting themselves and their families. Governments, institutions, and health care facilities all have a role in enacting policies that are respectful and inclusive of vulnerable populations when the nation is faced with a public health emergency such as the COVID-19 pandemic.
In the present context, the global COVID-19 pandemic has exacerbated existing health disparities and health care challenges and long-standing ethical issues that threaten the core values of the nursing profession ( Laurencin and McClinton, 2020 ; see Chapter 3 ). The roles nurses are playing to address these challenges are described throughout the report. On a positive note, however, the crisis of COVID-19 has brought much-needed attention to these challenges and has accelerated the adoption of tools and approaches for responding to them. For example, while telehealth has long been touted as a way to address issues of access to care, it took COVID-19 for clinicians, payers, and individuals to fully embrace it as a viable—and sometimes even preferred—alternative to in-person care ( Shah et al., 2020 ).
Before the COVID-19 pandemic, the United States was combatting the opioid overdose epidemic, which has led to devastating consequences that include opioid misuse, overdoses, and a rising number of newborns experiencing withdrawal syndrome due to parental opioid use and misuse during pregnancy ( NIH, 2021 ). Data for 2019 show that 70,630 people had died from drug overdose, 1.6 million had experienced an opioid use disorder, and 10.1 million had misused prescription opioids in the past year ( HHS, 2021 ). The opioid epidemic is a public health crisis that impacts both social and economic welfare, and its convergence with the COVID-19 pandemic has exacerbated health disparities and created new health care challenges that need to be addressed.
People of lower socioeconomic status, rural populations, and communities of color experience a higher burden of poor health relative to those of higher socioeconomic status, urban populations, and Whites, and the health inequity gap has been growing over time. Such inequities are unnecessary, unjust, and avoidable. The roots of these inequities are shaped by structural determinants, and understanding and acting on those determinants will help nurses play a pivotal role in improving health equity. Improving social conditions upstream and midstream has been found to have positive impacts on health status, and improving those conditions will likely reduce health inequities and improve the health of the U.S. population as a whole. Changes upstream through changes in national policy and midstream at the individual level through integrated social care are needed to connect individuals to social services that include healthy food, affordable housing, and transportation. As an example, although many other developed nations spend less per capita than the United States on medical services, they spend more on social services related to medical care, and their residents lead healthier lives ( NASEM, 2019a ). Addressing SDOH requires a community-oriented approach that involves aligning health care resources and investments to facilitate collaborations with community and government sectors, and bringing health care assets into broader advocacy activities that augment and strengthen social care resources ( NASEM, 2019a ).
This report focuses on how the next generation of nurses can contribute to efforts to address SDOH and achieve health equity if provided with appropriate resources, including education, training, and financial support. Later chapters will describe the relatively new efforts of nurses to address SDOH that have been enabled, for example, by new technologies, changes in payment models, and integration of social care.
Conclusion 2-1: Structural racism, cultural racism, and discrimination exist across all sectors, such as housing, education, criminal justice, employment, and health care, impacting the daily lives and health of individuals and communities of color. Nurses have a responsibility to address all of those forms of racism and to advocate for policies and laws that promote equity and the delivery of high-quality care to all individuals.
- Acker J, Braveman P, Arkin E, Leviton L, Parsons J, Hobor G. Mass incarceration threatens health equity in America. Princeton, NJ: Robert Wood Johnson Foundation; 2019.
- Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, Tweed EJ, Lewer D, Vittal Katikireddi S, Hayward AC. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: A systematic review and meta-analysis. Lancet. 2018; 391 (10117):241–250. [ PMC free article : PMC5803132 ] [ PubMed : 29137869 ]
- Amin K, Claxton G, Sawyer B, Cox C. How does cost affect access to care? Peterson-KFF Health System Tracker. 2019. [November 5, 2020]. https://www .healthsystemtracker .org/chart-collection /costaffect-access-care /#item-start .
- ANA (American Nurses Association). ANA’s membership assembly adopts resolution on racial justice for communities of color. 2020. [August 23, 2020]. https://www .nursingworld .org/news/news-releases /2020/ana-calls-for-racial-justice-for-communities-of-color .
- ANA Ethics Advisory Board. The nurse’s role in addressing discrimination: Protecting and promoting inclusive strategies in practice settings, policy, and advocacy. Online Journal of Issues in Nursing. 2019; 24 (3) doi: 10.3912/OJIN.Vol24No03PoSCol01.
- Armitage R, Nellums LB. Considering inequalities in the school closure response to COVID-19. Lancet Global Health. 2020; 8 (5):e644. [ PMC free article : PMC7195275 ] [ PubMed : 32222161 ]
- Artiga S, Orgera K, Damico A. Changes in health coverage by race and ethnicity since the ACA, 2010-2018. San Francisco, CA: Kaiser Family Foundation; 2020.
- Assari S. Social determinants of depression: The intersections of race, gender, and socioeconomic status. Brain Sciences. 2017; 7 (12) [ PMC free article : PMC5742759 ] [ PubMed : 29186800 ]
- Avery K, Finegold K, Xiao X. ASPE Issue Brief. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation; 2016. Impact of the Affordable Care Act coverage expansion on rural and urban populations.
- Balch B. It could have dire consequences for their health. Washington, DC: Association of American Medical Colleges; 2020. [January 4, 2021]. 54 million people in America face food insecurity during the pandemic. https://www .aamc.org /news-insights/54-million-people-america-face-food-insecurity-during-pandemic-it-could-have-dire-consequences-their .
- Barker AR, Nienstedt L, Kemper LM, McBride TD, Mueller KJ. Health insurance marketplaces: Issuer participation and premium trends in rural places, 2018. Rural Policy Brief. 2018; 2018 (3):1–4. [ PubMed : 30211515 ]
- Barnett ML, Lee D, Frank RG. In rural areas, buprenorphine waiver adoption since 2017 driven by nurse practitioners and physician assistants. Health Affairs. 2019; 38 (12):2048–2056. [ PMC free article : PMC6938159 ] [ PubMed : 31794302 ]
- Berger ZD, Evans NG, Phelan AL, Silverman RD. COVID-19: Control measures must be equitable and inclusive. BMJ. 2020; 368 :m1141. [ PubMed : 32198146 ]
- Bernardo CdeO, Bastos JL, González-Chica DA, Peres MA, Paradies YC. Interpersonal discrimination and markers of adiposity in longitudinal studies: A systematic review. Obesity Reviews. 2017; 18 (9):1040–1049. doi: 10.1111/obr.12564. [ PubMed : 28569010 ]
- Bharmal N, Derose KP, Felician M, Weden MM. Understanding the upstream social determinants of health. Santa Monica, CA: RAND Corporation; 2015.
- BLM (Black Lives Matter). Black Lives Matter: About. [March 4, 2021]. n.d. https: //blacklivesmatter.com/about .
- BLS (U.S. Bureau of Labor Statistics). Employment situation news release. 2020. [December 14, 2020]. https://www .bls.gov/news .release/archives/empsit_01082021 .htm .
- Boustan LP, Kahn ME, Rhode PW, Yanguas ML. The effect of natural disasters on economic activity in U.S. counties: A century of data. Cambridge, MA: National Bureau of Economic Research; 2017.
- Bovell-Ammon A, Mansilla C, Poblacion A, Rateau L, Heeren T, T .Cook J, Zhang T, de Cuba S, Sandel MT. Housing intervention for medically complex families associated with improved family health: Pilot randomized trial. Health Affairs (Millwood). 2020; 39 (4):613–621. [ PubMed : 32250672 ]
- Bowleg L. The problem with the phrase women and minorities: Intersectionality—an important theoretical framework for public health. American Journal of Public Health. 2012; 102 (7):1267–1273. [ PMC free article : PMC3477987 ] [ PubMed : 22594719 ]
- Braveman P, Acker J, Arkin E, Proctor D, Gillman A, McGeary KA, Mallya G. Wealth matters for health equity. Princeton, NJ: Robert Wood Johnson Foundation; 2018.
- Brinkley-Rubinstein L, Cloud DH. Mass incarceration as a social-structural driver of health inequities: A supplement to AJPH. American Journal of Public Health. 2020; 110 (51):S14–S16. [ PMC free article : PMC6987928 ] [ PubMed : 31967896 ]
- Caiola C, Barroso J, Docherty SL. Black mothers living with HIV picture the social determinants of health. Journal of the Association of Nurses in AIDS Care. 2018; 29 (2):204–219. [ PMC free article : PMC5816703 ] [ PubMed : 29273460 ]
- Carson EA. Prisoners in 2018. Washington, DC: U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics; 2020.
- Castrucci B, Auerbach J. Health Affairs Blog. 2019. Meeting individual social needs falls short of addressing social determinants of health. doi: 10.1377/hblog20190115.234942.
- CDC (Centers for Disease Control and Prevention). Rural health: Death (leading causes). 2017. [November 7, 2020]. https://www .cdc.gov/ruralhealth /cause-of-death.html .
- CDC. Prevalence of diagnosed diabetes. 2018. [March 15, 2021]. https://www .cdc.gov/diabetes /data/statistics-report /diagnosed-diabetes.html .
- CDC. COVID-19 hospitalization and death by race/ethnicity. 2020a. [August 27, 2020]. https://www .cdc.gov/coronavirus /2019-ncov /covid-data/investigations-discovery /hospitalization-death-by-race-ethnicity .html .
- CDC. CDC data show disproportionate COVID-19 impact in American Indian/Alaska Native populations. 2020b. [August 27, 2020]. https://www .cdc.gov/media /releases/2020/p0819-covid-19-impact-americanindian-alaska-native.html .
- G Cecil Sheps Center for Health Services Research. Rural hospital closures: More information. Chapel Hill: University of North Carolina; 2014a. [October 14, 2020]. https://www .shepscenter .unc.edu/programs-projects /rural-health /rural-hospital-closures-archive /rural-hospital-closures .
- G Cecil Sheps Center for Health Services Research. 176 rural hospital closures: January 2005—present (134 since 2010). Chapel Hill, NC: University of North Carolina; 2014b. [October 23, 2020]. https://www .shepscenter .unc.edu/programs-projects /rural-health /rural-hospital-closures .
- Chaturvedi R, Gabriel RA. Disaster Medicine and Public Health Preparedness. 2020. Coronavirus disease health care delivery impact on African Americans; pp. 1–3. doi: 10.1017/dmp.2020.179. [ PMC free article : PMC7298078 ] [ PubMed : 32466816 ]
- Chetty R, Hendren N. The impacts of neighborhoods on intergenerational mobility I: Childhood exposure effects. Quarterly Journal of Economics. 2018; 133 (3):1107–1162.
- Chetty R, Hendren N, Kline P, Saez E. Where is the land of opportunity? The geography of intergenerational mobility in the United States. Quarterly Journal of Economics. 2014; 129 (4):1553–1623.
- Chetty R, Stepner M, Abraham S, Lin S, Scuderi B, Turner N, Bergeron A, Cutler D. The association between income and life expectancy in the United States, 2001-2014. Journal of the American Medical Association. 2016; 315 (16):1750–1766. [ PMC free article : PMC4866586 ] [ PubMed : 27063997 ]
- Chou SC, Deng Y, Smart J, Parwani V, Bernstein SL, Venkatesh AK. Insurance status and access to urgent primary care follow-up after an emergency department visit in 2016. Annals of Emergency Medicine. 2018; 71 (4):487–496. [ PubMed : 29032870 ]
- Cole MB, Trivedi AN, Wright B, Carey K. Health insurance coverage and access to care for community health center patients: Evidence following the Affordable Care Act. Journal of General Internal Medicine. 2018; 33 (9):1444–1446. [ PMC free article : PMC6108997 ] [ PubMed : 29845464 ]
- Cruz D, Rodriguez Y, Mastropaolo C. Perceived microaggressions in health care: A measurement study. PLoS One. 2019; 14 (2) e0211620. [ PMC free article : PMC6363167 ] [ PubMed : 30721264 ]
- Cuellar NG, Aquino E, Dawson MA, Garcia-Dia MJ, Im EO, Jurado LM, Lee YS, Littlejohn S, Tom-Orme L, Toney DA. Culturally congruent health care of COVID-19 in minorities in the United States: A clinical practice paper from the National Coalition of Ethnic Minority Nurse Associations. Journal of Transcultural Nursing. 2020; 31 (5):434–443. [ PubMed : 32794439 ]
- Daly MC, Buckman SR, Seitelman LM. Federal Reserve Bank of San Francisco Economic Letter. 2020. The unequal impact of COVID-19: Why education matters; pp. 2020–17.
- Demain JG. Climate change and the impact on respiratory and allergic disease: 2018. Current Allergy and Asthma Reports. 2018; 18 (4):22. [ PubMed : 29574605 ]
- Dolezsar CM, McGrath JJ, Herzig AJM, Miller SB. Perceived racial discrimination and hypertension: A comprehensive systematic review. Health Psychology. 2014; 33 (1):20–34. [ PMC free article : PMC5756074 ] [ PubMed : 24417692 ]
- Escarce J. Health inequity in the United States: A primer. Philadelphia, PA: Penn Leonard Davis Institute of Health Economics; 2019.
- Fann N, Alman B, Broome RA, Morgan GG, Johnston FH, Pouliot G, Rappold AG. The health impacts and economic value of wildland fire episodes in the U.S.: 2008–2012. Science of the Total Environment. 2018; 610–611 :802–809. [ PMC free article : PMC6117838 ] [ PubMed : 28826118 ]
- FCC (Federal Communications Commission). Data: Broadband. 2015. [September 2, 2020]. https://www .fcc.gov/reportsresearch /maps /connect2health/data.html .
- FCC. Mapping broadband health in America. [September 2, 2020]. n.d. https://www .fcc.gov/health/maps .
- Fernandez-Lazaro CI, Adams DP, Fernandez-Lazaro D, Garcia-González JM, Caballero-Garcia A, Miron-Canelo JA. Medication adherence and barriers among low-income, uninsured patients with multiple chronic conditions. Research in Social and Administrative Pharmacy. 2019; 15 (6):744–753. [ PubMed : 30241872 ]
- FitzGerald C, Hurst S. Implicit bias in healthcare professionals: A systematic review. BMC Medical Ethics. 2017; 18 (1):19. [ PMC free article : PMC5333436 ] [ PubMed : 28249596 ]
- Foster K, Roche M, Delgado C, Cuzzillo C, Giandinoto JA, Furness T. Resilience and mental health nursing: An integrative review of international literature. International Journal of Mental Health Nursing. 2019; 28 (1):71–85. [ PubMed : 30294937 ]
- Garcia MC, Faul M, Massetti G, Thomas CC, Hong Y, Bauer UE, Iademarco MF. Reducing potentially excess deaths from the five leading causes of death in the rural United States. Morbidity and Mortality Weekly Report. 2017; 66 (2):1–7. [ PMC free article : PMC5829929 ] [ PubMed : 28081057 ]
- Garcia MA, Homan PA, García C, Brown TH. The color of COVID-19: Structural racism and the pandemic’s disproportionate impact on older racial and ethnic minorities. Journals of Gerontology, Series B. 2020; 76 (3):e75–e80. [ PMC free article : PMC7454923 ] [ PubMed : 32756973 ]
- Georgetown University Health Policy Institute. Rural and urban health. [September 2, 2020]. n.d. https://hpi .georgetown.edu/rural .
- Gordon K, Steele Gray C, Dainty KN, DeLacy J, Ware P, Seto E. Exploring an innovative care model and telemonitoring for the management of patients with complex chronic needs: Qualitative description study. Journal of Medical Internet Research Nursing. 2020; 3 (1):e15691. [ PMC free article : PMC8279442 ] [ PubMed : 34345777 ]
- Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Affairs. 2015; 34 (11):1830–1839. [ PubMed : 26526240 ]
- Hahn RA, Truman BI. Education improves public health and promotes health equity. International Journal of Health Services: Planning, Administration, Evaluation. 2015; 45 (4):657–678. [ PMC free article : PMC4691207 ] [ PubMed : 25995305 ]
- Hajat A, Kaufman JS, Rose KM, Siddiqi A, Thomas JC. Do the wealthy have a health advantage? Cardiovascular disease risk factors and wealth. Social Science & Medicine. 2010; 71 (11):1935–1942. [ PubMed : 20970902 ]
- Hall WJ, Chapman MV, Lee KM, Merino YM, Thomas TW, Payne BK, Eng E, Day SH, Coyne-Beasley T. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: A systematic review. American Journal of Public Health. 2015; 105 (12):e60–e76. [ PMC free article : PMC4638275 ] [ PubMed : 26469668 ]
- Henning-Smith C, Prasad S, Casey M, Kozhimannil K, Moscovice I. Rural-urban differences in Medicare quality scores persist after adjusting for sociodemographic and environmental characteristics. Journal of Rural Health. 2019; 35 (1):58–67. [ PubMed : 30561839 ]
- HHS (U.S. Department of Health and Human Services). Crude percent distributions (with standard errors) of type of health insurance coverage for persons under age 65 and for persons aged65 and over, by selected characteristics: United States, 2018. 2018. [March 15, 2021]. Table P-11c. https://ftp .cdc.gov/pub /Health_Statistics /NCHS/NHIS/SHS/2018_SHS_Table_P-11.pdf .
- HHS. Diabetes and African Americans. 2019. [October 20, 2020]. https: //minorityhealth .hhs.gov/omh/browse .aspx?lvl=4&lvlid=18 .
- HHS. Heart disease andAfrican Americans. 2020. [October 20, 2020]. https: //minorityhealth .hhs.gov/omh/browse .aspx?lvl=4&lvlid=19 .
- HHS. What is the U.S. opioid epidemic? 2021. [March 6, 2021]. https://www .hhs.gov/opioids /about-the-epidemic/index.html .
- Howell J, Elliott JR. Damages done: The longitudinal impacts of natural hazards on wealth inequality in the United States. Social Problems. 2018; 66 (3):448–467.
- Hudson DL, Bullard KM, Neighbors HW, Geronimus AT, Yang J, Jackson JS. Are benefits conferred with greater socioeconomic position undermined by racial discrimination among African American men? Journal of Men’s Health. 2012; 9 (2):127–136. [ PMC free article : PMC3371660 ] [ PubMed : 22707995 ]
- IFRC (International Federation of Red Cross and Red Crescent Societies). 2019. [March 15, 2021]. Heatwaves: Urgent action needed to tackle climate change’s “silent killer” https://media .ifrc.org /ifrc/pressrelease /heatwaves-urgent-action-needed-tackle-climate-changes-silent-killer .
- IPCC (Intergovernmental Panel on Climate Change). Managing the risks of extreme events and disasters to advance climate change adaptation: A special report of Working Groups I and II of the Intergovernmental Panel on Climate Change. Cambridge, UK: Cambridge University Press; 2012.
- Jividen S. Nurse.orgNurse.org. 2020. [November 6, 2020]. Nurses are going to protests, after work, to help injured people. https://nurse .org/articles /nurses-at-protests .
- Kantamneni N. Journal of Vocational Behavior. Vol. 119. 2020. The impact of the COVID-19 pandemic on marginalized populations in the United States: A research agenda; p. 103439. doi: 10.1016/j.jvb.2020.103439. [ PMC free article : PMC7205696 ] [ PubMed : 32390658 ]
- Killewald A, Pfeffer FT, Schachner JN. Wealth inequality and accumulation. Annual Review of Sociology. 2017; 43 :379–404. [ PMC free article : PMC5546759 ] [ PubMed : 28798522 ]
- Kim J, Richardson V. The impact of socioeconomic inequalities and lack of health insurance on physical functioning among middle-aged and older adults in the United States. Health & Social Care in the Community. 2012; 20 (1):42–51. [ PubMed : 21733029 ]
- Kinner SA, Young JT. Understanding and improving the health of people who experience incarceration: An overview and synthesis. Epidemiologic Reviews. 2018; 40 (1):4–11. [ PMC free article : PMC5982728 ] [ PubMed : 29860342 ]
- Landrine H, Corral I, Lee JG, Efird JT, Hall MB, Bess JJ. Residential segregation and racial cancer disparities: A systematic review. Journal of Racial and Ethnic Health Disparities. 2017; 4 (6):1195–1205. [ PubMed : 28039602 ]
- Laurencin CT, McClinton A. The COVID-19 pandemic: A call to action to identify and address racial and ethnic disparities. Journal of Racial and Ethnic Health Disparities. 2020; 7 (3):398–402. [ PMC free article : PMC7166096 ] [ PubMed : 32306369 ]
- Laws MB, Lee Y, Rogers WH, Beach MC, Saha S, Korthuis PT, Sharp V, Cohn J, Moore R, Wilson IB. Provider-patient communication about adherence to anti-retroviral regimens differs by patient race and ethnicity. AIDS and Behavior. 2014; 18 (7):1279–1287. [ PMC free article : PMC4047172 ] [ PubMed : 24464408 ]
- Levine DM, Landon BE, Linder JA. Quality and experience of outpatient care in the United States for adults with or without primary care. JAMA Internal Medicine. 2019; 179 (3):363–372. [ PMC free article : PMC6439688 ] [ PubMed : 30688977 ]
- Lewis TT, Williams DR, Tamene M, Clark CR. Self-reported experiences of discrimination and cardiovascular disease. Current Cardiovascular Risk Reports. 2014; 8 (1):1–15. [ PMC free article : PMC3980947 ] [ PubMed : 24729825 ]
- Lopez MH, Rainie L, Budiman A. Pew Research Center Factank. May 5, 2020. [September 2, 2020]. Financial and health impacts of COVID-19 vary widely by race and ethnicity. https://www .pewresearch .org/fact-tank/2020 /05/05/financial-and-health-impacts-of-covid-19-vary-widely-by-race-andethnicity .
- Lukachko A, Hatzenbuehler ML, Keyes KM. Structural racism and myocardial infarction in the United States. Social Science and Medicine. 2014; 103 :42–50. [ PMC free article : PMC4133127 ] [ PubMed : 24507909 ]
- Lundeen EA, Park S, Pan L, O’Toole T, Matthews K, Blanck HM. Obesity prevalence among adults living in metropolitan and nonmetropolitan counties—United States, 2016. Morbidity and Mortality Weekly Report. 2018; 67 (23):653. [ PMC free article : PMC6002035 ] [ PubMed : 29902166 ]
- Macinko J, Starfield B, Shi L. Quantifying the health benefits of primary care physician supply in the United States. International Journal of Health Services. 2007; 37 (1):111–126. [ PubMed : 17436988 ]
- Martsolf GR, Mason DJ, Soan J, Sullivan V. Nurse-designed care models: What can they tell us about advancing a culture of health? Santa Monica, CA: RAND Corporation; 2017.
- Massoglia M, Remster B. Linkages between incarceration and health. Public Health Reports. 2019; 134 (1)(Suppl):8S–14S. [ PMC free article : PMC6505320 ] [ PubMed : 31059410 ]
- McNutt M. Time’s up, CO2. Science. 2019; 365 (6452):411. [ PubMed : 31371582 ]
- Mehra R, Boyd LM, Ickovics JR. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Social Science & Medicine. 2017; 191 :237–250. [ PubMed : 28942206 ]
- Mesic A, Franklin L, Cansever A, Potter F, Sharma A, Knopov A, Siegel M. The relationship between structural racism and Black-White disparities in fatal police shootings at the state level. Journal of the National Medical Association. 2018; 110 (2):106–116. [ PubMed : 29580443 ]
- Mosites E, Parker EM, Clarke KEN, Gaeta JM, Baggett TP, Imbert E, Sankaran M, Scarborough A, Huster K, Hanson M, Gonzales E, Rauch J, Page L, McMichael TM, Keating R, Marx GE, Andrews T, Schmit K, Morris SB, Dowling NF, Peacock G., COVID Homelessness Team. Assessment of SARS-CoV-2 infection prevalence in homeless shelters—Four U.S. Cities, March 27–April 15, 2020. Morbidity and Mortality Weekly Report. 2020; 69 (17):521–522. [ PMC free article : PMC7206983 ] [ PubMed : 32352957 ]
- Moy E, Garcia MC, Bastian B, Rossen LM, Ingram DD, Faul M, Massetti GM, Thomas CC, Hong Y, Yoon PW, Iademarco MF. Leading causes of death in nonmetropolitan and metropolitan areas—United States, 1999–2014. Morbidity and Mortality Weekly Report. 2017; 66 (1):1–8. [ PMC free article : PMC5829895 ] [ PubMed : 28081058 ]
- Nadal KL, Griffin KE, Wong Y, Davidoff KC, Davis LS. The injurious relationship between racial microaggressions and physical health: Implications for social work. Journal of Ethnic & Cultural Diversity in Social Work. 2017; 26 (1–2):6–17.
- NASEM (National Academies of Sciences, Engineering, and Medicine). Communities in action: Pathways to health equity. Washington, DC: The National Academies Press; 2017. [ PubMed : 28418632 ]
- NASEM. Health-care utilization as a proxy in disability determination. Washington, DC: The National Academies Press; 2018. [ PubMed : 29782136 ]
- NASEM. Integrating social care into the delivery of health care: Moving upstream to improve the nation’s health. Washington, DC: The National Academies Press; 2019a. [ PubMed : 31940159 ]
- NASEM. Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. Washington, DC: The National Academies Press; 2019b. [ PubMed : 31855338 ]
- NASEM. Birth settings in America: Outcomes, quality, access, and choice. Washington, DC: National Academies Press; 2020. [ PubMed : 32049472 ]
- Nau C, Adams JL, Roblin D, Schmittdiel J, Schroeder E, Steiner JF. Considerations for identifying social needs in health care systems: A commentary on the role of predictive models in supporting a comprehensive social needs strategy. Medical Care. 2019; 57 (9):661–666. [ PubMed : 31404012 ]
- NCHS (National Center for Health Statistics). Health, United States, 2016: With chartbook on long-term trends in health. Hyattsville, MD: National Center for Health Statistics; 2017. Health, United States.
- NEJM (New England Journal of Medicine) Catalyst. Social determinants of health. 2017. [November 5, 2019]. https://catalyst .nejm .org/social-determinants-of-health .
- Newkirk V, Damico A. Kaiser Family Foundation. 2014. [September 2, 2020]. The Affordable Care Act and insurance coverage in rural areas. https://www .kff.org/uninsured /issue-brief /the-affordable-care-act-and-insurance-coverage-in-rural-areas .
- NIH (National Institutes of Health). Opioid overdose crisis. 2021. [March 6, 2021]. https://www .drugabuse .gov/drugtopics/opioids /opioid-overdose-crisis .
- NNU (National Nurses United). 2020. [November 6, 2020]. National Nurses United’s statement on protests and systemic racism: “Stop blaming underlying health conditions and comorbidities” https://www .nationalnursesunited .org/press /national-nurses-uniteds-statement-protests-and-systemic-racism .
- Odgers CL, Adler NE. Challenges for low-income children in an era of increasing income inequality. Child Development Perspectives. 2018; 12 (2):128–133.
- ODPHP (Office of Disease Prevention and Health Promotion). Social Determinants of Health. 2020a. [November 9, 2020]. https://www .healthypeople .gov/2020/topics-objectives /topic/social-determinants-of-health .
- ODPHP. Access to health services. 2020b. [November 9, 2020]. https://www .healthypeople .gov/2020/topics-objectives /topic/Access-to-Health-Services .
- Ong AD, Cerrada C, Williams DR, Lee RA. Stigma consciousness, racial microaggressions, and sleep disturbance among Asian Americans. Asian American Journal of Psychology. 2017; 8 (1):72–81.
- Owens A, Candipan J. Social and spatial inequalities of educational opportunity: A portrait of schools serving high- and low-income neighbourhoods in U.S. metropolitan areas. Urban Studies. 2019; 56 (15):3178–3197.
- Page KR, Venkataramani M, Beyrer C, Polk S. Undocumented U.S. immigrants and COVID-19. New England Journal of Medicine. 2020; 382 (21):e62. [ PubMed : 32220207 ]
- Paradies Y, Ben J, Denson N, Elias A, Priest N, Pieterse A, Gupta A, Kelaher M, Gee G. Racism as a determinant of health: A systematic review and meta-analysis. PLoS One. 2015; 10 (9) e0138511. [ PMC free article : PMC4580597 ] [ PubMed : 26398658 ]
- RHI (Rural Health Information Hub). Healthcare access in rural communities. 2020. [April 22, 2021]. https://www .ruralhealthinfo .org/topics/healthcare-access#faqs .
- Sasson I, Hayward MD. Association between educational attainment and causes of death among White and Black U.S. adults, 2010-2017. Journal of the American Medical Association. 2019; 322 (8):756–763. [ PMC free article : PMC6714034 ] [ PubMed : 31454044 ]
- Seo V, Baggett TP, Thorndike AN, Hull P, Hsu J, Newhouse JP, Fung V. Access to care among Medicaid and uninsured patients in community health centers after the Affordable Care Act. BMC Health Services Research. 2019; 19 (1):291. [ PMC free article : PMC6505197 ] [ PubMed : 31068205 ]
- Shah ED, Amann ST, Karlitz JJ. The time is now: A guide to sustainable telemedi-cine during COVID-19 and beyond. American Journal of Gastroenterology. 2020; 115 (9):1371–1375. [ PMC free article : PMC7382421 ] [ PubMed : 32694293 ]
- Shi L. The impact of primary care: A focused review. Scientifica. 2012; 2012 :432892. [ PMC free article : PMC3820521 ] [ PubMed : 24278694 ]
- Slopen N, Lewis TT, Williams DR. Discrimination and sleep: A systematic review. Sleep Medicine. 2016; 18 :88–95. [ PMC free article : PMC4699868 ] [ PubMed : 25770043 ]
- Solar O, Irwin A. A conceptual framework for action on the social determinants of health: Social determinants of health discussion paper 2. Geneva, Switzerland: World Health Organization; 2010.
- Sue DW, Capodilupo CM, Torino GC, Bucceri JM, Holder AM, Nadal KL, Esquilin M. Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist. 2007; 62 (4):271–286. [ PubMed : 17516773 ]
- Supekar S. Equitable resettlement for climate change-displaced communities in the United States. UCLA Law Review. 2019; 66 :1290.
- Taylor LA. Health Affairs Health Policy Brief. 2018. Housing and health: An overview of the literature. doi: 10.1377/HPB20180313.396577.
- USDA (U.S. Department of Agriculture). Food security and nutrition assistance. 2020. [September 2, 2020]. https://www .ers.usda .gov/data-products/ag-and-food-statistics-charting-the-essentials /food-security-andnutrition-assistance .
- van Dorn A, Cooney RE, Sabin ML. COVID-19 exacerbating inequalities in the U.S. Lancet. 2020; 395 (10232):1243–1244. [ PMC free article : PMC7162639 ] [ PubMed : 32305087 ]
- van Ryn M, Burke J. The effect of patient race and socio-economic status on physicians’ perceptions of patients. Social Science & Medicine. 2000; 50 (6):813–828. [ PubMed : 10695979 ]
- Wallis C. Why racism, not race, is a risk factor for dying of COVID-19. Scientific American: Public Health. Jun 12, 2020. [November 6, 2020]. https://www .scientificamerican .com/article /why-racism-not-race-is-a-risk-factor-for-dying-of-COVID-191 .
- Weissman J, Pratt LA, Miller EA, Parker JD. Serious psychological distress among adults: United States, 2009–2013. Hyattsville, MD: National Center for Health Statistics; 2015.
- Williams DR, Lawrence JA, Davis BA. Racism and health: Evidence and needed research. Annual Review of Public Health. 2019; 40 :105–125. [ PMC free article : PMC6532402 ] [ PubMed : 30601726 ]
- Woolf SH, Aron L, Dubay L, Simon SM, Zimmerman E, Luk KX. Urban Institute and Virginia Commonwealth University Center on Society and Health. 2015. How are income and wealth linked to health and longevity?
- Yancy CW. COVID-19 and African Americans. Journal of the American Medical Association. 2020; 323 (19):1891–1892. [ PubMed : 32293639 ]
- Zagorsky JL, Smith PK. Does asthma impair wealth accumulation or does wealth protect against asthma? Social Science Quarterly. 2016; 97 (5):1070–1081.
Black Lives Matter is a global organization whose mission is “to eradicate white supremacy and build local power to intervene in violence inflicted on Black communities by the state and vigilantes” ( BLM, n.d. ).
- Cite this Page National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on the Future of Nursing 2020–2030; Flaubert JL, Le Menestrel S, Williams DR, et al., editors. The Future of Nursing 2020-2030: Charting a Path to Achieve Health Equity. Washington (DC): National Academies Press (US); 2021 May 11. 2, Social Determinants of Health and Health Equity.
- PDF version of this title (5.6M)
In this Page
Related information.
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Social Determinants of Health and Health Equity - The Future of Nursing 2020-203... Social Determinants of Health and Health Equity - The Future of Nursing 2020-2030
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
COMMENTS
The role of social motivational factors in health and ill health. To be able to understand the social motivational factors in health and ill health, we must understand how sociology differs and compares to the biomedical aspect of care. The social model focuses on the social impacts of health such as income, education and environment alongside ...
The diagram below was illustrated by Dahlgreen and Whitehead to show how all the factors fit together to help policy makers and health care workers understand how social factors influence health, called the social model of health. The diagram shows a range of factors that create health inequalities and inequities.
Reading Time: 5 minutes. Social factors in health and social care encompass a range of elements that influence the wellbeing of individuals and communities. These factors are critical in understanding the holistic needs of patients and service users. Here we will delve into some key social factors and their impact on health and social care.
Health is determined by several factors including genetic inheritance, personal behaviors, access to quality health care, and the general external environment (such as the quality of air, water, and housing conditions). In addition, a growing body of research has documented associations between social and cultural factors and health (Berkman and Kawachi, 2000; Marmot and Wilkinson, 2006).
Abstract. During the past two decades, the public health community's attention has been drawn increasingly to the social determinants of health (SDH)—the factors apart from medical care that can be influenced by social policies and shape health in powerful ways. We use "medical care" rather than "health care" to refer to clinical ...
Introduction and background. According to the World Health Organization (WHO), social determinants of health (SDH) are defined as the circumstances in which humans are born, develop, live, earn, and age. At the international, regional, and state or local levels, the distribution of money, power, and resources shapes these circumstances [ 1 ].
Social Factors in Health and Social Care. START COURSE DETAILS. Caret pointing down. Course Outline. Three vertical lines aligned to the left. Unit Introduction. A circle with a colored border representing one's progress through a lesson. sociological factors influencing the relationships between patients and health professionALS ...
Table 13.1 "Theory Snapshot" summarizes what they say. Good health and effective medical care are essential for the smooth functioning of society. Patients must perform the "sick role" in order to be perceived as legitimately ill and to be exempt from their normal obligations.
Social determinants of health are the conditions in which people are born, grow, live, work and age.1 They include factors like socioeconomic status, education, neighborhood and physical ...
Social determinants of health fall into five broad groups:. Healthcare: This group encompasses a person's access to healthcare and its quality. Factors include: access to primary healthcare ...
The social determinants of health (SDH) are the non-medical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life. These forces and systems include economic policies and systems, development agendas, social ...
Lindsey Kirkby Unit 11 Social Factors in Health and Social care Throughout life, people are continuously building their own social support networks just by participating in daily activities, this can include meeting colleagues at work, befriending somebody at the gym, or even just having a chat on their daily commute. However, for the elderly it can be more difficult to build a social network ...
Social determinants of health (SDOH) are the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks. SDOH can be grouped into 5 domains: Economic Stability. Education Access and Quality. Health Care Access and Quality.
Sociological factors influencing the relationship between patients and health professionals. Social factors like doctor-patient interaction influencing the relationship between patients and health professionals can be classified as microsociology because it deals with smaller sites of interactions. There are sociological factors that affect patient-doctor relationship and these factors have ...
Background Addressing health disparities is necessary to ensure appropriate care for patients. This study examined the impact of Clinical Week experiences on students' recognition of social determinants of health early in their medical education. Methods A 5-day experience each of the first three semesters of medical school provided direct patient care experiences. Two Clinical Weeks were ...
A health care disparity typically refers to differences between groups in health insurance coverage, affordability, access to and use of care, and quality of care. The terms "health inequality ...
The central tenet of Bandura's social-cognitive theory is that people seek to develop a sense of agency and exert control over the important events in their lives. This sense of agency and control is affected by factors such as self-efficacy, outcome expectations, goals, and self-evaluation (Schunk, 2012).
Social Determinants of Health (SDOH): A Brief Overview. There are many factors that influence our health. These factors are referred to as determinants of health. One kind of determinant of health is what is in our genes and our biology. Another determinant is our individual behavior, which include choices we make, such as smoking, exercise ...
Abstract. Health behaviors shape health and well-being in individuals and populations. Drawing on recent research, we review applications of the widely applied "social determinants" approach to health behaviors. This approach shifts the lens from individual attribution and responsibility to societal organization and the myriad institutions ...
Building a healthier future for all. Healthy People 2030 sets data-driven national objectives to improve health and well-being over the next decade. Healthy People 2030 includes 359 core — or measurable — objectives as well as developmental and research objectives. Learn more about the types of objectives.
Stark racial disparities in maternal and infant health in the U.S. have persisted for decades despite continued advancements in medical care. The disparate impact of the COVID-19 pandemic for ...
Healthy People 2030 focuses on improving health by helping people get timely, high-quality health care services. About 1 in 10 people in the United States don't have health insurance.1 People without insurance are less likely to have a primary care provider, and they may not be able to afford the health care services and medications they need.
Background Social and Therapeutic Horticulture (STH) is a process where trained practitioners work with plants and people to improve an individual's physical and psychological health, communication and thinking skills. Evidence suggests that STH can support individuals with mental ill-health, however, current commissioning of STH within mental health care is limited. This study aimed to ...
Health and social care; Public health; ... Topics covered have been chosen to include a broad range of conditions, health outcomes and risk factors for poor health and wellbeing. These topics will ...
Research shows that factors such as income, education level, where you live, and the type of job you have, as well as stressors on the job may raise your risk of high blood pressure. Working early or late shifts is one example of a social factor that can raise your risk. Experiencing discrimination and poverty has been linked to high blood ...
This research is funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme, conducted through the Policy Research Unit in Maternal and Neonatal Health and Care, PR-PRU-1217-21202. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
SOCIAL DETERMINANTS OF HEALTH. The growing evidence for inequities in both health and access to health care has brought added scrutiny to SDOH. The term typically refers to "nonmedical factors influencing health, including health-related knowledge, attitudes, beliefs, or behaviors" (such as smoking) (Bharmal et al., 2015, p. 2).Examples of SDOH also include education, employment, health ...