- Open access
- Published: 11 June 2015

“Down syndrome: an insight of the disease”
- Ambreen Asim 1 ,
- Ashok Kumar 1 ,
- Srinivasan Muthuswamy 1 ,
- Shalu Jain 1 &
- Sarita Agarwal 1
Journal of Biomedical Science volume 22 , Article number: 41 ( 2015 ) Cite this article
165k Accesses
171 Citations
16 Altmetric
Metrics details
Down syndrome (DS) is one of the commonest disorders with huge medical and social cost. DS is associated with number of phenotypes including congenital heart defects, leukemia, Alzeihmer’s disease, Hirschsprung disease etc. DS individuals are affected by these phenotypes to a variable extent thus understanding the cause of this variation is a key challenge. In the present review article, we emphasize an overview of DS, DS-associated phenotypes diagnosis and management of the disease. The genes or miRNA involved in Down syndrome associated Alzheimer’s disease, congenital heart defects (AVSD), leukemia including AMKL and ALL, hypertension and Hirschprung disease are discussed in this article. Moreover, we have also reviewed various prenatal diagnostic method from karyotyping to rapid molecular methods - MLPA, FISH, QF-PCR, PSQ, NGS and noninvasive prenatal diagnosis in detail.
Introduction
Down syndrome is one of the most leading causes of intellectual disability and millions of these patients face various health issues including learning and memory, congenital heart diseases(CHD), Alzheimer’s diseases (AD), leukemia, cancers and Hirschprung disease(HD). The incidence of trisomy is influenced by maternal age and differs in population (between 1 in 319 and 1 in 1000 live births) [ 1 - 5 ]. DS has high genetic complexity and phenotype variability [ 6 - 8 ]. Trisomic fetuses are at elevated risk of miscarriages and DS people have increased incidence of developing several medical conditions [ 9 ]. Recent advancement in medical treatment with social support has increased the life expectancy for DS population. In developed countries, the average life span for DS population is 55 years [ 10 ].
Various conditions associated with Downs’s syndrome with its causative genes.
Human Chromosome 21
DS complex phenotype results from dosage imbalance of genes located on human chromosome 21(Hsa 21). The genetic nature of DS together with the relatively small size of Hsa 21 encouraged scientist to concentrate efforts towards the complete characterization of this chromosome in the past few years. The length of 21q is 33.5 Mb [ 11 ] and 21 p is 5–15 Mb [ 12 ]. A total 225 genes was estimated when initial sequence of 21q was published [ 11 ]. Hsa 21 has 40.06% repeat content out of which the repeat content of SINE’s, LINE’s, and LTR are 10.84%, 15.15%, 9.21% respectively. The Table 1 given below highlights some of the genes present on chromosome 21.
Features of DS
There are various conserved features occurring in all DS population, including learning disabilities, craniofacial abnormality and hypotonia in early infancy [ 13 ]. Some people of DS are affected by variant phenotypes including atrioventricular septal defects (AVSD) in heart, leukemia’s (both acute megakaryoblastic leukemia(AMKL) and acute lymphoblastic leukemia(ALL)), AD and HD. DS individual have variety of physical characteristics like a small chin, slanted eye, poor muscle tone, a flat nasal bridge, a single crease of the palm and a protuding due to small mouth and large tongue [ 14 ]. Other features includes big toe, abnormal pattern of fingerprint and short fingers.
Genetics of the disease
The most common cause of having a DS babies is presence extra copy chromosome 21 resulting in trisomy. The other causes can be Robertsonian translocation and isochromosomal or ring chromosome. Ischromosome is a term used to describe a condition in which two long arms of chromosome separate together rather than the long and short arm separating together during egg sperm development. Trisomy 21 (karyotype 47, XX, + 21 for females and 47, XY, + 21 for males) is caused by a failure of the chromosome 21 to separate during egg or sperm development. In Robertsonian translocation which occurs only in 2-4% of the cases, the long arm of the chromosome 21 is attached to another chromosome (generally chromosome 14). While mosaicism deals with the error or misdivision occurs after fertilization at some point during cell division. Due to this people with mosaic DS have two cell lineages which contribute to tissues and organs of individuals with Mosacism (one with the normal number of chromosomes, and other one with an extra number 21) [ 15 ].
Genotype-phenotype correlation
Gene dosage imbalance hypothesis states that DS patients have an increased dosage or copy number of genes on Hsa 21 that may lead to an increase in gene expression [ 13 - 15 ]. This hypothesis has been extended to include the possibility that specific genes or subsets of genes may control specific DS phenotypes [ 16 ]. Amplified developmental instability hypothesis states that a non-specific dosage of a number of trisomic genes leads to a genetic imbalance that causes a great impact on the expression and regulation of many genes throughout the genome [ 13 , 14 ]. Another hypothesis known as critical region hypothesis was also added to this list. Phenotypic analyses was done on individuals with partial trisomy for Hsa21 identified that only one or a few small chromosomal regions, termed “Down syndrome critical regions” (DSCR) a region of 3.8-6.5 Mb on 21q21.22, with approximately 30 genes responsible for the majority of DS phenotypes [ 15 , 16 ]. Previously a region of 1.6 to 2.5 Mb was recognised as sufficient cause for DS pehnotype [17, 18]. The sequencing of Hsa 21 proved to be an important factor in the progression of DS research [ 19 ] and led to further insight into genotype-phenotype correlations associated with DS and precise characterizations of DSCR regions [ 13 ]. A “critical region” within 21q22 was believed to be responsible for several DS phenotypes including craniofacial abnormalities, congenital heart defects of the endocardial cushions, clinodactyly of the fifth finger and mental retardation [ 20 ].
Dual-specificity tyrosine phosphorylation-regulated kinase (DYRK1A) and regulator of calcineurin 1 (RCAN1), Down syndrome cell adhesion molecule (DSCAM) has been suggested to play a critical role in the developing brain and has also been identified as a candidate gene for the increased risk of CHD in DS individuals [ 21 , 22 ]. DSCAM is a critical factor in neural differentiation, axon guidance, and the establishment of neural networks and it has been suggested that the disruption of these processes contributes to the DS neurocognitive phenotype [ 22 ]. Based on thorough analyses of studies on humans and DS mouse models, it is evident that there is not a single critical region of genes sufficient to cause all DS phenotypes. Alternatively, it is likely that there are multiple critical regions or critical genes contributing to a respective phenotype or group of phenotypes associated with DS [ 23 ].
Various clinical conditions associated to Down syndrome
The various clinical conditions associated with DS are Alzheimer’s disease, heart defects, leukemia, hypertension and gastrointestinal problems (Figure 1 ). The molecular pathogenesis mechanism of these DS related phenotype must be studied along with its causative agents in order to have a better understanding of the disease. Below are some DS related phenotype discussed in detail which are as follows:
Neurological problems
DS patients have greatly increased risk of early onset AD. After the age of 50, the risk of developing dementia increases in DS patients up to 70% [ 23 - 27 ]. There are various genes reported to cause early onset AD. Some of the genes described in the current literature are APP (amyloid precursor protein), BACE2 (beta secretase 2), PICALM (Phosphatidylinositol binding clathrin assembly protein) and APOE(Apolipoprotein E) etc. APP is an integral membrane protein which is concentrated in synapse of neurons and trisomy of this protein is likely to make significant contribution to the increased frequency of dementia in DS individuals. The triplication of Hsa 21 along with APP in people without DS has been recently shown to be associated with early onset AD. A tetranucleotide repeat, ATTT , in intron 7 of the amyloid precursor protein has been associated with the age of onset of AD in DS in a preliminary study [ 28 ]. Various mouse models are used to observe degeneration of basal forebrain cholinergic neurons (BFCNs). Ts65Dn mice is dependent on trisomy of APP expression of retrograde axonal transport [ 29 ]. Studies have also revealed that BACE2 which encodes enzyme beta secretase 2 is also involved in AD. APP and BACE 2 genes are located on chromosome 21. The current data on DS support the association of haplotypes in BACE2 with AD [ 30 ]. Besides APP and BACE2 genes, other genes like PICALM and APOE are also found to be associated with the age of onset of Alzheimer’s dimentia in DS [ 31 ].
Cardiac problems
The incidence of CHD in newborn babies with DS is up to 50% [ 32 ]. Endocardial cushion defect also called as atrioventricular cushion defect is most common form which affects up to 40% of the patients. Ventricular septal defect (VSD) is also present in these population which affects up to 35% of the patients [ 33 ]. The essential morphological hallmark of an AVSD is the presence of a common atrioventricular junction as compared to the separate right and left atrioventricular junction in the normal heart. Other morphological features include defects of the muscular and membranous atrioventricular septum and an ovoid shape of the common atrioventricular junction. There is disproportion of outlet and inlet dimensions of the left ventricle, with the former greater than the latter as compared to the normal heart where both dimensions are similar [ 34 ]. While in case of VSD, the defect lies in ventricular septum of the heart due to which some of the blood from the left ventricle leaks into the right ventric leading to pulmonary hypertension. Mutation in non Hsa 21 CRELD1 (Cysteine rich EGF like domain1) gene contributes to the development of AVSD in DS [ 35 ]. CRELD1 is located on chromosome 3p25. It encodes a cell surface protein that functions as cell adhesion molecule and is expressed during cardiac cushion development. CRELD1 gene contains 11 exons spanning approximately 12 kb [ 36 ]. To the present, two specific genetic loci for AVSD have been identified. One was AVSD 1 locus present on chromosome 1p31-p21 [ 37 ]. Other locus was present on chromosome 3p25 and the corresponding gene was CRELD1 [ 36 , 38 ]. Maslen et al . in [ 33 ] have identified two heterozygous missense mutation (p.R329C and p.E414K) with two subjects in DS and AVSD. They have recruited 39 individual of DS with complete AVSD and have found the same mutations. In the same study, DNA of 30 individual of trisomy without CHD was studied for both mutations, no such mutation was identified [ 35 ]. R329C which was originally reported in an individual with sporadic partial AVSD and now it is also detected in individual of DS with AVSD. Interestingly, with the same mutation (p.R329C), the severity of heart defect was greater in patients of DS with AVSD. Thus, identification of CRELD 1 mutation in 2/39 individual (5.1%) of DS with complete AVSD suggests the defects in CRELD 1 contribute to pathogenesis of AVSD in context with trisomy 21.
Hematological problems
Patients with DS display a unique spectrum of malignancies, which include leukemia’s as well as solid tumors. The first report of leukemia in a DS patient occurred in 1930 [ 39 ] and the first systematic study in 1957 [ 40 ]. Studies indicate that patients with DS have a 10–20 fold increased relative risk of leukemia, with a cumulative risk of 2% by age 5 and 2.7% by age 30 [ 41 ]. They constitute approximately 2% of all pediatric acute lymphoblastic leukemia(ALL) and approximately 10% of pediatric acute myeloid leukemia (AML). Leukemogenesis of acute megakaryoblastic leukemia (AMKL) in DS patients is associated with the presence of somatic mutations involving GATA 1 gene (or also called as GATA-binding factor 1) [ 42 ]. GATA 1 is a chromosome X- linked transcription factor which is essential for erythoid and megakaryocytic differentiation. Because of these GATA 1 mutations, there is a production of shorter GATA 1 protein thereby leading to uncontrolled proliferation of immature megakaryocytes [ 42 , 43 ]. On the other hand, acquired gain of function mutation in Janus Kinase 2 gene are present in approximately 30% of cases with ALL in DS [ 44 , 45 ].
Hypertension
People with DS have been reported to have a reduced incidence of hypertension [ 46 , 47 ]. Trisomy of the Hsa21 microRNA hsa-miR-155 contributes to this [ 48 ]. Hsa-miR-155 is proposed to specifically target one allele of the type-1 angiotensin II receptor (AGTR1) gene, resulting in it’s under- expression, which contribute to a reduced risk of hypertension. Further studies are required to validate this hypothesis and determine whether other genes may also protect people with DS against hypertension.
Gastrointestinal problems
DS patients constitute ~12% of all cases of HD. Duodenal stenosis (DST) and imperforate anus (IA) are 260 and 33 times more likely to occur DS [ 23 , 49 ]. HD is a form of low intestinal obstruction caused by the absence of normal myenteric ganglion cells in a segment of the colon [ 50 ]. In HD children, the absence of ganglion cells results in the failure of the distal intestine to relax normally. Peristaltic waves do not pass through the aganglionic segment and there is no normal defecation, leading to functional obstruction. Abdominal distention, failure to pass meconium, enterocolitis and bilious vomiting are the predominant signs and symptoms and appear within a few days after birth. Infants with duodenal atresia or DST present with bilious vomiting early in the neonatal period. If left untreated, it will result in severe dehydration and electrolyte imbalance. IA is a birth defects in which the rectum is malformed and it is associated with an increased incidence of some other specific anomalies as well, together being called the VACTERL association: vertebral anomalies, anal atresia, cardiovascular anomalies, tracheoesophageal fistula, esophageal atresia, renal and limb defects.
Alterations of approximately 10 non Hsa21 genes have been linked to this disease [ 51 ]. Several researches have shown that HD contain the DSCAM gene which is expressed in neural crest that give rise to enteric nervous system [ 49 ]. Overlapping critical region was described both for DST and IA [ 51 ]. No other Hsa21 genes have been implicated so far.
Diagnostic methods
Prevention of DS depends upon offering prenatal diagnosis to high risk pregnancies via amniocentesis and chorionic villus sampling (CVS). Amniocentesis and CVS are quite reliable but offers risk of miscarriage of between 0.5 to 1% [ 52 ]. Based soft markers like small or no nasal bone, large ventricles and nuchal fold thickness, the risk of DS for fetus can be identified through ultrasound generally at 14 to 24 weeks of gestation [ 53 ]. Increased fetal nuchal translucency indicates an increased risk of DS [ 54 ]. The other methods used for prenatal diagnosis in which traditional cytogenic analysis is still widely used in different countries. However some rapid molecular assays-FISH(fluorescent in situ hybridization), QF-PCR (quantitative fluorescence PCR), and MLPA(multiplex probe ligation assay)- also used for prenatal diagnosis.
Routine karyotyping
Cytogenetic analysis of metaphase karyotype remains the standard practice to identify not only trisomy 21, but also all other aneuploidies and balanced translocations. Details on diagnostic methods with advantages and disadvantages are mentioned in Table 2 .
Rapid aneuploidy testing methods
Over the past 10 years however, several other methods have been developed and used for the rapid detection of trisomy 21, either in fetal life or after birth. The most widely used is FISH of interphase nuclei, using Hsa 21-specific probes or whole-Hsa 21 [ 55 ]. An alternative method that is now widely used in some countries is QF-PCR, in which DNA polymorphic markers (microsatellites) on Hsa 21 are used to determine the presence of three different alleles [ 56 ]. This method relies on informative markers and the availability of DNA. Rapid diagnosis by PCR-based methods using polymorphic STR markers may reduce these difficulties using conventional approach. Using STR markers method we can detect trisomy in 86.67% cases with only two markers. Using more number of markers can further increase the reliability of the test. Simultaneously parental origin of the nondysjunction can also be detected [ 57 , 58 ]. Additional method to measure copy number of DNA sequences include MLPA [ 59 ] which was first introduced in 2002 as a method of relative quantification in DNA. MLPA offers various advantages like – a very short time for diagnosis (2–4 days), effectiveness, simplicity and relatively low costs. It is based on hybridization and PCR method and is divided into four steps: DNA denaturation, hybridization of probe to the complementary target sequence, probe ligation and PCR amplification. And finally capillary electrophoresis of PCR amplified products is carried out. However MLPA is unable to exclude low level placental and true mosaicism [ 60 ].
Advancement in the diagnosis
A recent method, termed paralogous sequence quantification (PSQ), uses paralogous sequences to quantify the Hsa 21 copy number. PSQ is a PCR based method for the detection of targeted chromosome number abnormalities termed paralogous sequence quantification (PSQ), based on the use of paralogous genes. Paralogous sequences have a high degree of sequence identity, but accumulate nucleotide substitutions in a locus specific manner. These sequence differences, which are termed as paralogous sequence mismatches (PSMs), can be quantified using pyrosequencing technology, to estimate the relative dosage between different chromosomes. PSQ is a robust, easy to interpret, and easy to set up method for the diagnosis of common aneuploidies, and can be performed in less than 48 h, representing a competitive alternative for widespread use in diagnostic laboratories. The sequencing is quantitatively done by using pyrosequencing [ 61 ]. Finally, comparative genomic hybridization (CGH) on BAC chips can be used for the diagnosis of full trisomy or monosomy, and for partial (segmental) aneuploidies [ 62 , 63 ].
Noninvasive Prenatal diagnosis
Fetal cells in maternal ciruculation: Ever since the discovery of presence of fetal lymphocytes in maternal blood was made in 1969, the investigators are trying to develop genetics-based noninvasive prenatal diagnostics (NIPD) [ 64 ]. Despite several advantages offered by this approach, the use of fetal cells for NIPD has never reached clinical implementation because of their paucity (on the order of a few cells per milliliter of maternal blood) and concerns of fetal cell persistence in the maternal circulation between pregnancies.
Cell free fetal DNA from maternal serum: This novel approach was proposed in 1997. Cell-free fetal DNA constitutes between 5% and 10% of the total DNA in maternal plasma and increases during gestation and rapidly clears from the circulation post delivery. Several clinical applications based on the analysis of cell-free fetal DNA have been developed like determining fetal Rh D status in Rh D-negative women [ 65 ], sex in sex-linked disorders [ 66 , 67 ], and detection of paternally inherited autosomal recessive and dominant mutations [ 68 ]. However, there remains the outstanding challenge of the use of cell-free fetal DNA for the detection of chromosomal aneuploidy, in particular trisomies 21, 18, and 13. Several approaches have been adopted like the origin of circulating cell-free fetal DNA is primarily the placenta, whereas maternal cell-free DNA is derived from maternal leukocytes [ 69 ]. The approach includes studying differences in genomic DNA methylation between the placenta and paired maternal leukocytes, investigators have characterized placenta-specific epigenetic markers [ 70 ] and also finding of circulating cell-free placenta-derived mRNA allowed the identification of placenta-specific mRNA production [ 71 ].
The concept of digital PCR was also introduced to serve the same purpose. In digital PCR, individual fetal and maternal circulating cell-free DNA fragments are amplified under limiting-dilution conditions and the total number of chromosome 21 amplifications (representing maternal plus fetal contributions) divided by the number of reference chromosome amplifications should yield a ratio indicating an over- or underrepresentation of chromosome 21.
Although the digital PCR approach is conceptually solid, the low percentage of cell-free fetal DNA in the maternal plasma sample requires the performance of thousands of PCRs to generate a ratio with statistical confidence. This can be overcome by using of multiple target amplifications and enrichment of cell-free fetal DNA which are still under research trail.
Next recent method added to the list is next generation sequencing (NGS) which is based on the principle of clonally amplified DNA templates (or, most recently, single DNA molecules) are sequenced in a massively parallel fashion within a flow cell [ 72 , 73 ]. NGS provides digital quantitative information, in which each sequence read is a countable “sequence tag” representing an individual clonal DNA template or a single DNA molecule. This quantification allows NGS to expand the digital PCR concept of counting cell-free DNA molecules.
Fan et al. and Chiu et al. in 2008 described noninvasive detection of trisomy 21 by NGS [ 74 ]. Both groups extracted cell-free DNA from maternal plasma samples from both euploid and trisomy pregnancies. DNA from each sample was sequenced on the Illumina Genome Analyzer, and each sequence read was aligned to the reference human genome. Chiu et al. build on their earlier work with the Illumina Genome Analyzer and demonstrate noninvasive NGS-based trisomy 21 detection with the sequencing-by-ligation approach on the Life Technologies SOLiD platform [ 75 ]. Cell-free DNA was extracted from 15 pregnant women, 5 of whom carried trisomy 21 fetuses and it was clonally amplified by emulsion PCR, and sequenced in 1 chamber of an 8-chamber SOLiD slide. This process yielded a median of 59 × 10 6 50-base reads per sample. A median of 12 × 10 6 reads (or 21%) were each aligned uniquely to one location of the reference human genome (with masking of repeat regions), for a coverage of approximately 20% of the haploid human genome. For each trisomy 21 case, the chromosome 21 z score value indicated a 99% chance of a statistically significant difference from the chromosome 21 z scores for the controls. As reported earlier with the Illumina Genome Analyzer, a nonuniform distribution of aligned sequence reads was observed with the SOLiD data.
The current time for sample processing, sequencing, and data interpretation in experienced hands is 5 to 8 days for the Genome Analyzer and SOLiD platforms respectively with the cost of approximately $700 – $1000 per sample. Going forward, one can expect streamlining and automation of technical processes and data analysis, coupled with reduced sequencing costs.
Ultimately, reduced sequencing costs and turnaround times could pave the way for NGS-based NIPD to be considered as an alternative to serum biomarker screening, which,while cost-effective remains prone to false positives. Forty years after the discovery of circulating fetal cells, the vision of NIPD appears clearer and closer.
Management of the disease
One of the hallmarks of DS is the variability in the way that the condition affects people with DS. With the third 21st chromosome existing in every cell, it is not surprising to find that every system in the body is affected in some way. However, not every child with DS has the same problems or associated conditions. Parents of children with DS should be aware of these possible conditions so they can be diagnosed and treated quickly and appropriately. The goal of the study is to point out the most common problems of which parents should be aware.
Timely surgical treatment of cardiac defects during first 6 months of life may prevent from serious complications. Congenital cataracts occur in about 3% of children and must be extracted soon after birth to allow light to reach the retina. A balance diet and regular exercise are needed to maintain appropriate weight. Feeding problems and failure to thrive usually improve after cardiac surgery. A DS child should have regular check up from various consultants. These include:
Clinical geneticist - Referral to a genetics counseling program is highly desirable
Developmental pediatrician
Cardiologist - Early cardiologic evaluation is crucial for diagnosing and treating congenital heart defects, which occur in as many as 60% of these patients
Pediatric pneumonologist -Recurrent respiratory tract infections are common in patients with DS
Ophthalmologist
Neurologist/Neurosurgeon – As many as 10% of patients with DS have epilepsy; therefore, neurologic evaluation may be needed
Orthopedic specialist
Child psychiatrist - A child psychiatrist should lead liaison interventions, family therapies, and psychometric evaluations
Physical and occupational therapist
Speech-language pathologist
Audiologist
DS or Trisomy 21, being the most common chromosomal abnormality among live born infants, is associated with a number of congenital malformations. Several theories have been put forward to increase our understanding in phenotype and genotype correlation. A “critical region” within 21q22 was believed to be responsible for several DS phenotypes including craniofacial abnormalities, congenital heart defects of the endocardial cushions, clinodactyly of the fifth finger and mental retardation and several other features. The primary goal of this review is to unravel the common genes involved in DS associated phenotypes, including APP, BACE2, PICALM, APOE, GATA 1, JAK 2, CRELD 1 and DSCAM. This reviews also provides the detailed description on the application of techniques to prenatal diagnosis in DS. Rapid aneuploidy testing has been introduced in mid 1990’s in the form of FISH where testing can be done on uncultured amniocytes. Within a couple of years, MLPA and QF-PCR has been added in the list of rapid aneuploidy testing. The other methods includes: NGS for cell free fetal DNA screening for maternal plasma. Except ,FISH, MLPA and QF-PCR other method are not commercialized for aneuploidy diagnosis due to their running cost, labor intensive protocol and complex data analysis. Since various clinical conditions are associated with DS, hence the management of these patients requires an organized multidisciplinary approach and continuous monitoring of these patients which has been discussed in this review article.
O’ Nuallain S, Flanagan O, Raffat I, Avalos G, Dineen B. The prevalence of Down syndrome in County Galway. Ir Med. 2009;100:329–31.
Google Scholar
Carothers AD, Hecht CA, Hook EB. International variation in reported live birth prevalence rates of Down syndrome, adjusted for maternal age. J Med Genet. 1999;36:386–93.
Canfield MA, Honein MA, Yuskiv N, Xing J, Mai CT, Collins JS, et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States. Birth Defects Res A Clin Mol Teratol. 2006;76:747–56.
Murthy SK, Malhotra AK, Mani S, Shara ME, Al Rowaished EE, Naveed S, et al. Incidence of Down syndrome in Dubai. Med Princ Pract. 2007;16:25–8.
Article PubMed Google Scholar
Wahab AA, Bener A, Teebi AS. The incidence patterns of Down syndrome in Qatar. Clin Genet. 2006;69:360–2.
Mégarbané A, Ravel A, Mircher C, Sturtz F, Grattau Y, Rethoré MO et al. The 50th anniversary of the discovery of trisomy 21: the past, present, and future of research and treatment of Down syndrome. Genet Med. 2009;11:611–6.
Gardiner KJ. Molecular basis of pharmacotherapies for cognition in Down syndrome. Trends Pharmacol Sci. 2010;31:66–73.
Article CAS PubMed Central PubMed Google Scholar
Prandini P, Deutsch S, Lyle R, Gagnebin M, Delucinge Vivier C, Delorenzi M et al. Natural gene-expression variation in Down syndrome modulates the outcome of gene-dosage imbalance. Am J Hum Genet. 2007;81:252–63.
Morris JK, Wald NJ, Watt HC. Fetal loss in Down syndrome pregnancies. Prenat Diagn. 1999;19:142–5.
Article CAS PubMed Google Scholar
Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD, Bittles AH, et al. The changing survival profile of people with Down’s syndrome: implications for genetic counselling. Clin Genet. 2002;62:390–3.
Lyle R, Bena F, Gagos S, Gehrig C, Lopez G, Schinzel A, et al. Genotype–phenotype correlations in Down syndrome identified by array CGH in 30 cases of partial trisomy and partial monosomy chromosome 21. Eur J Hum Genet. 2009;17:454–66.
Ermak G, Harris CD, Battocchio D, Davies KJ. RCAN1 (DSCR1 or Adapt78) stimulates expression of GSK-3beta. FEBS J. 2006;273:2100–9.
Antonarakis SE, Lyle R, Dermitzakis ET, Reymond A, Deutsch S. Chromosome 21 and Down syndrome: from genomics to pathophysiology. Nat Rev Genet. 2004;5:725–38.
Sinet PM, Theopile D, Rahmani Z, Chettouch Z, Blovin JL, Prier M, et al. Mapping of Down syndrome phenotype on chromosome 21 at the molecular level. Biomed Pharmacother. 1994;48(5–6):247–52.
Epstein CJ, Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The Metabolic & Molecular Bases of Inherited Disease. New York: McGraw-Hill; 2001. p. 1223–56.
Pritchard MA, Kola I. The "gene dosage effect" hypothesis versus the "amplified developmental instability" hypothesis in Down syndrome. J Neural Transm Suppl. 1999;57:293–303.
CAS PubMed Google Scholar
Patterson D. Genetic mechanisms involved in the phenotype of Down syndrome. Ment Retard Dev Disabil Res Rev. 2007;13:199–206.
Shapiro BL. Down syndrome–a disruption of homeostasis. Am J Med Genet. 1983;14:241–69.
Delabar JM, Theophile D, Rahmani Z, Chettouh Z, Blouin JL, Prieur M, et al. Molecular mapping of twenty-four features of Down syndrome on chromosome 21. Eur J Hum Genet. 1993;1:114–24.
Ohira M, Ichikawa H, Suzuki E, Iwaki M, Suzuki K, Saito-Ohara F, et al. A 1.6-Mb P1-based physical map of the Down syndrome region on chromosome 21. Genomics. 1996;33:65–74.
Korbel JO, Tirosh-Wagner T, Urban AE, Chen XN, Kasowski M, Dai L, et al. The genetic architecture of Down syndrome phenotypes revealed by high-resolution analysis of human segmental trisomies. Proc Natl Acad Sci U S A. 2009;106:12031–6.
Niebuhr E. Down's syndrome. The possibility of a pathogenetic segment on chromosome no. 21. Humangenetik. 1974;21:99–101.
Holland AJ, Hon J, Huppert FA, Stevens F. Incidence and course of dementia in people with Down’s syndrome: findings from a population-based study. J Intellect Disabil Res. 2000;44:138–46.
Holland AJ, Hon J, Huppert FA, Stevens F, Watson P. Population-based study of the prevalence and presentation of dementia in adults with Down’s syndrome. Br J Psychiatry. 1998;172:493–8.
Janicki MP, Dalton AJ. Prevalence of dementia and impact on intellectual disability services. Ment Retard. 2000;38:276–88.
Johannsen P, Christensen JE, Mai J. The prevalence of dementia in Down syndrome. Dementia. 1996;7:221–5.
Lai F, Williams RS. A prospective study of Alzheimer disease in Down syndrome. Arch Neurol. 1989;46:849–53.
EL Jones, CG Ballard, VP Prasher, M Arno, S Tyrer, B Moore et al. An Intron 7 polymorphism in APP affects the age of Dimentia in Down Syndrome. Int J Alzheimers Dis. 2011;5. doi:10.4061/2011/929102
Salehi A, Delcroix JD, Belichenko PV, Zhan KWC, Valletta JS, Takimoto-Kimura, et al. Increased App expression in a mouse model of Down’s syndrome disrupts NGF transport and causes cholinergic neuron degeneration. Neuron. 2006;51:29–42.23.
Myllykangas L, Wavrant –De Vrieze F, Polvikoski T, Notkola IL, Sulkava R, Niinisto L. Chromosome 21 BACE2 haplotype associates with Alzheimer's disease: a two-stage study. J Neurol Sci. 2005;236(1–2):17–24.
Jones EL, Mok K, Hanney M, Harold D, Sims R, Williams J. Evidence that PICALM affects age at onset of Alzheimer’s dementia in Down syndrome. Neurobiol Aging. 2013;34(10):244.
Article Google Scholar
Urbano R. Health issues among person with down syndrome. 2012.
Maslen CL, Babcock D, Robinson SW, Bean LJ, Dooley KJ, Willour VL, et al. CRELD1 mutations contribute to the occurrence of cardiac atrioventricular septal defects in Down syndrome. Am J Med Genet. 2006;140:2501–5.
Craig B. Atrioventricular septal defect: from fetus to adult. Heart. 2006;92(12):1879–85.
Article PubMed Central PubMed Google Scholar
Rup PA, Fouad GT, Egelston CA, Reifsteck CA, Oslon SB, Knosp WM, et al. Identification, genomic organization and mRNA expression of CRELD1, the founding member of a unique family of matricellular proteins. Gene. 2002;293:47–57.
Sheffield VC, Pierpont ME, Nishimura D, Beek JS, Burns TL, Berg MA, et al. Identification of a complex congenital heart defect susceptibility locus by using DNA pooling and shared segment analysis. Hum Mol Genet. 1997;6:117–21.
Priestley MD, Water J, Maliszewska C, Latif F, Maher ER. Detailed mapping of a congenital heart disease gene in chromosome 3p25. J Med Genet. 2000;37:581–7.
Robinsom SW, Morris CD, Goldmuntz E, Reller MD, Jones MA, Maslen CL, et al. Missense mutation in CRELD1 are associated with cardiac atrioventricular septal defects. Am J Hum Genet. 2003;72:1047–52.
Brewster HF, Cannon HE. Acute lymphatic leukemia: Report of a case in eleventh month mongolina idiot. New Orleans Med Surg J. 1930;82:872–3.
Krivit W, Good RA. Simultaneous occurrence of mongolism and leukemia; report of a nationwide survey. AMA J Dis Child. 1957;94:289–93.
Hasle H, Clemmensen IH, Mikkelsen M. Risks of leukaemia and solid tumours in individuals with Down’s syndrome. Lancet. 2000;355:165–9.
Wechsler J, Greene M, McDevitt MA, Anastasi J, Karp JE, Le Beau MM, et al. Acquired mutations in GATA1 in the megakaryoblastic leukemia of Down syndrome. Nat Genet. 2002;32(1):148–52.
Shivdasani RA, Fujiwara Y, McDevitt MA, Orkin SH. A lineage-selective knockout establishes the critical role of transcription factor GATA-1 in megakaryocyte growth and platelet development. EMBO J. 1997;16(13):3965–73.
Kearney L, Gonzalez De Castro D, Yeung J, Procter J, Horsley SW, Eguchi-Ishimae M, et al. Specific JAK2 mutation (JAK2R683) andmultiple gene deletions in Down syndrome acute lymphoblastic leukemia. Blood. 2009;113(3):646–8.
Morrison RA, McGrath A, Davidson G, Brown JJ, Murray GD, Lever AF. Low blood pressure in Down’s syndrome, a link with Alzheimer’s disease? Hypertension. 1996;28:569–75.
Draheim CC, McCubbin JA, Williams DP. Differences in cardiovascular disease risk between nondiabetic adults with mental retardation with and without Down syndrome. Am J Ment Retard. 2002;107:201–11.
Sethupathy P, Borel C, Gagnebin M, Grant GR, Deutsch S, Elton TS, et al. Human microRNA-155 on chromosome 21 differentially interacts with its polymorphic target in the AGTR1 3’ untranslated region: a mechanism for functional single-nucleotide polymorphisms related to phenotypes. Am J Hum Genet. 2007;81:405–13.
Torfs CP, Christianson RE. Anomalies in Down syndrome individuals in a large population-based registry. Am J Med Genet. 1998;77:431–8.
Berrocal T, Lamas M, Gutiérrez J. Congenital Anomalies of the Small Intestine, Colon, and Rectum. Radiographics Radiol Bras. 1999;19:1219–36.
Article CAS Google Scholar
Amiel J, Sproat-Emison E, Garcia-Barcelo M, Lantieri F, Burzynski G, Borrego S, et al. Hirschsprung disease, associated syndromes and genetics: a review. J Med Genet. 2008;45:1–14.
Tabor A, Alfirevic Z. Update on procedure-related risks for prenatal diagnosis techniques. Fetal Diagn Ther. 2010;27(1):1–7.
Reena MS, Pisani PO Conversano F, Perrone E, Casciaro E, Renzo GCD et al. Sonographic markers for early diagnosis of fetal malformations. World J Radiol. 2013;10:356-371.
Agathokleous M, Chaveeva P, Poon LC, Kosinski P, Nicolaides KH. Meta-analysis of second-trimester markers for trisomy 21. Ultrasound Obstetrics Gynecol. 2013;41(3):247–61.
F.D. Malone, M.E D'Alton. First trimester sonographic screenign for Down syndrome. Obstetrics and Gynecology. 2003;102:1066-79.
Kuo WL. Detection of aneuploidy involving chromosomes 13, 18, or 21, by fluorescence in situ hybridization (FISH) to interphase and metaphase amniocytes. Am J Hum Genet. 1991;49:112–9.
CAS PubMed Central PubMed Google Scholar
Shalu J, Sarita A, Inusha P, Parag T, Shubha P. Diagnosis of Down Syndrome and Detection of Origin of Nondisjunction by Short Tandem Repeat Analysis. Genetic Test Mol Biomark. 2010;14:4.
Shalu J, Inusha P, Shubha RP, Sarita A. Multiplex quantitative fluorescent polymerase chain reaction for detection of aneuploidies. Genet Test Mol Biomarker. 2012;16:624–7.
Armour JA, Sismani C, Patsalis PC, Cross G. Measurement of locus copy number by hybridisation with amplifiable probes. Nucleic Acids Res. 2000;28:605–9.
Slater HR, Bruno DL, Ren H, Pertile M, Schouten JP, Choo KH. Rapid, high throughput prenatal detection of aneuploidy using a novel quantitative method (MLPA). J Med Genet. 2003;40:907–12.
Van Veghel-Plandsoen M, Wouters C, Kromosoeto J. Multiplex ligation-dependent probe amplification is not suitable for detection of low-grade mosaicism. Eur J Hum Genet. 2011;19:1009–12.
S Deutsch, U Choudhury, SE Antonarakis. Detection of trisomy 21 and other aneuploidies by paralogous gene quantification. J Med Genet (in the press).
Ishkanian AS, Malloff CA, Watson SK, DeLeeuw RJ, Chi B, Coe BP. A tiling resolution DNA microarray with complete coverage of the human genome. Nature Genet. 2004;36:299–303.
Snijders AM, Nowak N, Segraves R, Blackwood S, Brown N, Conroy J et al. Assembly of microarrays for genome- wide measurement of DNA copy number. Nature Genet. 2001;29:263–4.
Walknowska J, Conte FA, Grumbach MM. Practical and theoretical implications of fetal- maternal lymphocyte transfer. Lancet. 1969;1:1119–22.
Daniels G, Finning K, Martin P, Massey E. Noninvasive prenatal diagnosis of fetal blood group phenotypes: current practice and future prospects. Prenat Diagn. 2009;29:101–7.
Lo YM, Corbetta N, Chamberlain PF, Rai V, Sargent IL, Redman CW, et al. Presence of fetal DNA in maternal plasma and serum. Lancet. 1997;350:485–7.
Costa JM, Benachi A, Gautier E. New strategy for prenatal diagnosis of X-linked disorders. N Engl J Med. 2002;346:1502.
Wright CF, Burton H. The use of cell-free fetal nucleic acids in maternal blood for non-invasive prenatal diagnosis. Hum Reprod Update. 2009;15:139–51.
Alberry M, Maddocks D, Jones M, Abdel Hadi M, Abdel-Fattah S, Avent N, et al. Free fetal DNA in maternal plasma in anembryonic pregnancies: confirmation that the origin is the trophoblast. Prenat Diagn. 2007;27:415–8.
Chim SS, Jin S, Lee TY, Lun FM, Lee WS, Chan LY, et al. Systematic search for placental DNA-methylation markers on chromosome 21: toward a maternal plasma-based epigenetic test for fetal trisomy 21. Clin Chem. 2008;54:500–11.
Mardis ER. The impact of next-generation sequencing technology on genetics. Trends Genet. 2008;24:133–41.
Voelkerding KV, Dames SA, Durtschi JD. Next-generation sequencing: from basic research to diagnostics. Clin Chem. 2009;55:641–58.
Fan HC, Blumenfeld YJ, Chitkara U, Hudgins L, Quake SR. Noninvasive diagnosis of fetal aneuploidy by shotgun sequencing DNA from maternal blood. Proc Natl Acad Sci U S A. 2008;105:16266–71.
Chiu RW, Chan KC, Gao Y, Lau VY, Zheng W, Leung TY, et al. Noninvasive prenatal diagnosis of fetal chromosomal aneuploidy by massively parallel genomic sequencing of DNA in maternal plasma. Proc Natl Acad Sci U S A. 2008;105:20458–63.
Chiu RWK, Sun H, Akolekar R, Clouser C, Lee C, McKernan K, et al. Maternal plasma DNA analysis with massively parallel sequencing by ligation for noninvasive prenatal diagnosis of trisomy 21. Clin Chem. 2010;56:459–63.
Download references
Author information
Authors and affiliations.
Department of Medical Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, 226014, India
Ambreen Asim, Ashok Kumar, Srinivasan Muthuswamy, Shalu Jain & Sarita Agarwal
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Sarita Agarwal .
Additional information
Competing interests.
The authors declare that they have no competing interests.
Authors' contribution
AA drafting of the manuscript, AS and MS, did substantial contribution in finalising, correcting and critical review of manuscript, KA and JS contributed in review and collection of articles. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/ .
The Creative Commons Public Domain Dedication waiver ( https://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Asim, A., Kumar, A., Muthuswamy, S. et al. “Down syndrome: an insight of the disease”. J Biomed Sci 22 , 41 (2015). https://doi.org/10.1186/s12929-015-0138-y
Download citation
Received : 28 May 2014
Accepted : 22 April 2015
Published : 11 June 2015
DOI : https://doi.org/10.1186/s12929-015-0138-y
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Down Syndrome
- Imperforate Anus
- Illumina Genome Analyzer
- Endocardial Cushion
- Down Syndrome Patient
Journal of Biomedical Science
ISSN: 1423-0127
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
Home — Essay Samples — Nursing & Health — Other Diseases & Conditions — Down Syndrome
Essay Examples on Down Syndrome
Down syndrome essay topics and outline examples, essay title 1: embracing diversity: understanding down syndrome, its causes, and challenges.
Thesis Statement: This essay aims to provide a comprehensive understanding of Down syndrome, including its genetic causes, associated health challenges, and the importance of inclusion and support for individuals with Down syndrome.
- Introduction
- Defining Down Syndrome: An Overview of Trisomy 21
- Genetic Causes: Understanding the Extra Chromosome 21
- Health Challenges: Physical and Intellectual Characteristics of Down Syndrome
- Early Intervention and Education: Strategies for Optimal Development
- Inclusive Society: The Importance of Acceptance and Equal Opportunities
- Supportive Networks: Families, Advocacy Groups, and Healthcare
- Conclusion: Celebrating the Abilities and Contributions of Individuals with Down Syndrome
Essay Title 2: Breaking Stereotypes: Achievements, Success Stories, and Opportunities for People with Down Syndrome
Thesis Statement: This essay explores the accomplishments and potential of individuals with Down syndrome, highlighting success stories, educational achievements, and the broader societal impact of challenging stereotypes.
- Historical Perspectives: Changing Attitudes Towards Down Syndrome
- Education and Employment: Navigating Opportunities and Challenges
- Success Stories: Remarkable Achievements of Individuals with Down Syndrome
- Fostering Independence: Life Skills and Empowerment Programs
- Family Perspectives: The Role of Supportive Parents and Siblings
- Changing Perceptions: The Impact of Advocacy and Awareness Campaigns
- Conclusion: Redefining What's Possible for People with Down Syndrome
Essay Title 3: Advances in Down Syndrome Research: Genetics, Therapies, and Future Prospects
Thesis Statement: This essay delves into the realm of Down syndrome research, highlighting recent developments in genetics, therapeutic approaches, and the potential future directions that hold promise for improving the quality of life for individuals with Down syndrome.
- Genetic Insights: Discoveries in Trisomy 21 Research
- Therapeutic Strategies: Speech, Occupational, and Physical Therapies
- Cognitive Development: Enhancing Learning and Communication
- Early Intervention: The Importance of Early Diagnosis and Support
- Future Directions: Emerging Technologies and Innovative Research Areas
- Global Collaboration: International Efforts to Improve Down Syndrome Care
- Conclusion: The Promising Path Towards Enhanced Quality of Life for Individuals with Down Syndrome
Down Syndrome: Causes, Symptoms, and Support
The causes and physical and mental effects of down syndrome, made-to-order essay as fast as you need it.
Each essay is customized to cater to your unique preferences
+ experts online
The Speech and Language Deficits of Children with Down Syndrome
Case study on corrective surgical procedure, paternal age: the considerable confounding risk factor in chromosomal aneuploidies, why cosmetic surgery is not an answer to down syndrome, let us write you an essay from scratch.
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Relevant topics
- Atherosclerosis
- Hearing Loss
- Infertility
- Eating Disorders
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free
93 Down Syndrome Essay Topic Ideas & Examples
🏆 best down syndrome topic ideas & essay examples, ⭐ good research topics about down syndrome, 📃 simple & easy down syndrome essay titles, ❓ research questions about down syndrome.
- Children Diagnosed with Down Syndrome Down syndrome is a condition that can occur in any child of any family, and this makes it indispensable for everyone to have information regarding the condition.
- Down’s Syndrome Recurrence Discussion A 30-year-old mother has a 1 in 1000 chance of giving birth to a child with Down’s syndrome. When reducing the risk of 1 in 1000 by three, it is possible to calculate an increasing […]
- Prenatal Testing for Down Syndrome The key points of contention in the discussion are the justification of the risks, the ethical choice on the principle of health, and the responsibility for stigmatization.
- The Down Syndrome Impacts on the Body Face morphology and upper nasal mucosa infections are the primary causes of chronic ear problems in newborns with Down syndrome. Developmental delays and behavioral issues in youngsters with Down syndrome are common.
- Down Syndrome in Karyotype Studies Frequent external manifestations of the disease are the flattened face, almond-shaped, the tongue that tends to stick out of the mouth.
- Challenges of Families with Down Syndrome Children The first challenge that the White family encountered was the decision of what to do with the fetus. It was only after the birth that Herzenbergs knew that the child had Down syndrome, while Whites […]
- Down Syndrome Genetics and Behaviors Using current research literature on behavioral issues and novel treatments for Down syndrome, this paper explores and discusses behavioral inflexibility, restrictive and repetitive behaviors, and Down syndrome’s neurogenetic nature.
- Down Syndrome: Prenatal Testing, Chronic Health Conditions, and Cognitive Deficits Its purpose is to “test the validity and reliability of a scale that measures pregnant women’s attitudes and decision-making concerning prenatal Down syndrome screening and diagnosis in urban areas of Taiwan”.
- Comprehensive Care Plan for Patients with Down Syndrome It may also be highly beneficial to evaluate significant events that may influence the physical and mental health of the patient.
- Maternal Serum and Down Syndrome The main purpose of the research is to identify the authors who considered the problem of Down’s syndrome causes and analyze the results of the research conducted by those scholars.
- Down Syndrome’s Symptoms and Effects on Learning Abilities in Students At the same time, the woman’s age of 35 and older is considered a risk factor that increases the chance of Down syndrome in the baby.
- The Great Down-Aging Syndrome: Why 40 Is the New 20 It has also been observed that the middle-aged people are fervent consumers of those products that are mainly used by the young. Not all middle-aged consumers are attracted to products that are meant for the […]
- Blunt Abdominal Trauma in Down Syndrome Patient Delving into the case, we could also admit the fact that the usage of the given examination procedure helped to determine the signs of Systemic inflammatory response syndrome, which could be extremely dangerous for the […]
- Down Syndrome: Education and Life Possibilities DS is one of the foremost causes of cognitive impairment in children; however, with early interventions and medical advances, the potential for individuals with DS is expanding by the day.
- Pregnancy Termination in Down’s Syndrome Case One of the reasons why women of different ages decide to terminate their pregnancy is any genetic disease of the fetus and the risk of having an unhealthy child.
- Down Syndrome as the Most Common Genetic Condition in the US Firstly, to describe Down syndrome and the life of people with this disorder, it is necessary to give a scientific definition to this condition and underline the causes. People with Down syndrome are also people, […]
- Down Syndrome in the UAE: Attitude of Society and Family Healthy influence of these mammals is proved and the UAE tries to create the best conditions for people who suffer from Down Syndrome.
- Child with Down’s Syndrome – Life Story After playing for a while, he followed us to the living room, and I was moved to tears when he took my hand into his and asked my name.
- Down Syndrome and Dementia: Theories and Treatment The genetic material in the chromosome 21 is responsible for the development of the disorder, and its symptoms appear at the infantry stage of development.
- Mental Development in Children With Down Syndrome Mental development in children with Down syndrome varies greatly and at birth, it is not possible to predict the extent to which the child will be affected in terms of physical symptoms and cognitive development.
- Learners with Down Syndrome: A Handbook for Teaching Professionals The research premises on a set of research studies to provide experimental evaluation of current programs that address education of children with disabilities.
- Types of Tests Identifying Down Syndrome The major cause of the syndrome is associated with the existence of extra copy of the 21st chromosome. The triple screen test serves to identify Down syndrome in cases the level of AFP is low […]
- Living With the Down Syndrome: Causes and Symptoms
- Corrigendum: Pioglitazone Improves Mitochondrial Organization and Bioenergetics in Down Syndrome Cells
- Microstate Changes Associated With Alzheimer’s Disease in Persons With Down Syndrome
- Low-Resolution Place and Response Learning Capacities in Down Syndrome
- Genetics and Evolution: Cystic Fibrosis and Down Syndrome
- The Speech and Language Deficits of Children With Down Syndrome
- Inclusive Classrooms With Down Syndrome Students
- Autism, Down Syndrome and Equal Rights: A Look at the Past and Present of Diverse Populations and Sport
- Down Syndrome and Spina Bifida – Cause, Effects and Treatment
- Down Syndrome and the Value of Inclusive Education
- Response Inhibition and Interference Suppression in Individuals With Down Syndrome Compared to Typically Developing Children
- Semantic Verbal Fluency Pattern, Dementia Rating Scores and Adaptive Behavior Correlate With Plasma A 42 Concentrations in Down Syndrome Young Adults
- Music Therapy and Down Syndrome
- Between ‘Desperation’ and Disability Rights: Analysis of Alternative Medicine for Children With Down Syndrome
- Chromosomal Abnormalities: Down Syndrome
- Health Issues, Diabetes and Down Syndrome
- Problems Associated With Children With Down Syndrome
- Psychological and Physical Characteristics of Down Syndrome
- Most Successful People Who Have Down Syndrome
- Down Syndrome Affects Physical Growth, Facial Characteristics
- Cognitive Skills, Behavior and Learning Potential of Preschool Children With Down Syndrome
- The Causes, Symptoms, Diagnosis and Management of Down Syndrome
- Children With Down Syndrome: A Developmental Disorder
- Down Syndrome and the Formation of Reproductive Cells
- Down Syndrome Children Interaction With Family and Peers
- Causation and Developmental Course of Down Syndrome
- Dance Therapy for Down Syndrome Effects and Improvements
- Classroom Behaviour, Language Competence, and the Acceptance of Children With Down Syndrome by Their Mainstream Peers
- Learning Styles for Children With Down Syndrome
- The Negative and Positive Influence of the Media on People With Down Syndrome
- Parents and Children With Birth Defects: Down Syndrome
- Children With Intellectual Disabilities: Down Syndrome
- Down Syndrome: Causes, Symptoms, Diagnosis, & Treatment
- Development and Learning for People With Down Syndrome
- The Physical and Mental Characteristics of Children With Down Syndrome, Increased Risk Factors, and the Need for Medical Care and Stimulating Environments
- Maternal Line-1 DNA Methylation and Congenital Heart Defects in Down Syndrome
- Health Case History: Down Syndrome and Moderate Intellectual Disability
- Blood Beta-Amyloid and Tau in Down Syndrome: A Comparison With Alzheimers Disease
- Improving Working Memory Abilities in Individuals With Down Syndrome: A Treatment Case Study
- Allocentric Spatial Learning and Memory Deficits in Down Syndrome
- What Causes Down Syndrome?
- Why the Family Physician Patient Patients With Down Syndrome?
- How Does Down Syndrome Affect the One Who Has It?
- How Can Individuals With Down Syndrome Prosper in Life?
- How Do Individuals With Down Syndrome Process Faces and Words Conveying Emotions?
- Which Gender Is More Likely to Get Down Syndrome?
- What Is Down’s Syndrome Caused By?
- Can a Down Syndrome Girl Have a Baby?
- What Are the Five Characteristics of Down Syndrome?
- What Is the Life Expectancy of a Down Syndrome Person?
- Can Down Syndrome Be Cured?
- What Are the Three Types of Down Syndrome?
- How Can You Prevent Down Syndrome During Pregnancy?
- Can People With Down Syndrome Be Smart?
- What Happens if the Down Syndrome Test Is Positive?
- Does Down Syndrome Run in the Family?
- Is Autism a Form of Down Syndrome?
- Can Stress Cause Down Syndrome?
- Can Two Down Syndromes Have a Normal Baby?
- Is Down Syndrome a Disability?
- Which Organ Is Most Often Affected by Down Syndrome?
- Does a Mother’s Age Affect Down Syndrome?
- Can You Tell if a Baby Has Down Syndrome in an Ultrasound?
- What Is the Most Common Cause of Death in Down Syndrome?
- Can a Person With Down Syndrome Drive?
- Who Is the Oldest Person With Down Syndrome?
- What Are the Symptoms of Down Syndrome in Pregnancy?
- Can Down Syndrome Be Cured During Pregnancy?
- What Race Is Down Syndrome Most Common In?
- What Week of Pregnancy Does Down Syndrome Occur?
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2024, February 26). 93 Down Syndrome Essay Topic Ideas & Examples. https://ivypanda.com/essays/topic/down-syndrome-essay-topics/
"93 Down Syndrome Essay Topic Ideas & Examples." IvyPanda , 26 Feb. 2024, ivypanda.com/essays/topic/down-syndrome-essay-topics/.
IvyPanda . (2024) '93 Down Syndrome Essay Topic Ideas & Examples'. 26 February.
IvyPanda . 2024. "93 Down Syndrome Essay Topic Ideas & Examples." February 26, 2024. https://ivypanda.com/essays/topic/down-syndrome-essay-topics/.
1. IvyPanda . "93 Down Syndrome Essay Topic Ideas & Examples." February 26, 2024. https://ivypanda.com/essays/topic/down-syndrome-essay-topics/.
Bibliography
IvyPanda . "93 Down Syndrome Essay Topic Ideas & Examples." February 26, 2024. https://ivypanda.com/essays/topic/down-syndrome-essay-topics/.
- Abnormal Psychology Paper Topics
- BPD Research Ideas
- Epigenetics Essay Titles
- Dyslexia Topics
- Bipolar Disorder Research Ideas
- Genetic Engineering Topics
- Nervous System Research Topics
- Parenting Research Topics
Your Privacy on DSE sites
We use cookies to provide essential functionality and to analyse how our sites are used.
We work to discover how and why development differs for children with Down syndrome, and how we can best help them to achieve their potential.
We support scientific research that advances our understanding of the development of children and young people with Down syndrome across many aspects of development, including cognition, memory, speech, language, reading and numeracy.
Our research has repeatedly demonstrated that children with Down syndrome can achieve more when given appropriate opportunities and effective support.

Advancing understanding for over 45 years
For over 45 years, we have conducted and supported innovative research, working in close collaboration and partnership with families and scientists around the world.
Our research has delivered important insights into speech and language, memory, reading, number and mathematics, social skills, education, sleep and behaviour for children with Down syndrome.
Today, this research guides many thousands of families, professionals and organisations, helping them provide better support, therapy and education for children and young people with Down syndrome in over 100 countries.
Down Syndrome Research Forum 2025
DSE hosts the annual Down Syndrome Research Forum, bringing researchers, students, practitioners and families together to discuss current research and practice.
The Down Syndrome Research Forum 2024 was held on 25 and 26 April. We expect to announce the dates for the Down Syndrome Research Forum 2025 soon.
- Research and Practice
- News and Update
Presentations
- Research Forum
- Online courses
- See and Learn
Legal information
- Cookies Policy
- Privacy Policy
- Terms of Use
- Terms of sale
- DSE Client ID
- Access RLI Online
- Subscriptions
- English (Australia)
- English (Canada)
- English (India)
- English (Ireland)
- English (Malaysia)
- English (New Zealand)
- English (Philippines)
- English (Singapore)
- English (South Africa)
- English (United Kingdom)
- English (United States)
- Undergraduate
- High School
- Architecture
- American History
- Asian History
- Antique Literature
- American Literature
- Asian Literature
- Classic English Literature
- World Literature
- Creative Writing
- Linguistics
- Criminal Justice
- Legal Issues
- Anthropology
- Archaeology
- Political Science
- World Affairs
- African-American Studies
- East European Studies
- Latin-American Studies
- Native-American Studies
- West European Studies
- Family and Consumer Science
- Social Issues
- Women and Gender Studies
- Social Work
- Natural Sciences
- Pharmacology
- Earth science
- Agriculture
- Agricultural Studies
- Computer Science
- IT Management
- Mathematics
- Investments
- Engineering and Technology
- Engineering
- Aeronautics
- Medicine and Health
- Alternative Medicine
- Communications and Media
- Advertising
- Communication Strategies
- Public Relations
- Educational Theories
- Teacher's Career
- Chicago/Turabian
- Company Analysis
- Education Theories
- Shakespeare
- Canadian Studies
- Food Safety
- Relation of Global Warming and Extreme Weather Condition
- Movie Review
- Admission Essay
- Annotated Bibliography
- Application Essay
- Article Critique
- Article Review
- Article Writing
- Book Review
- Business Plan
- Business Proposal
- Capstone Project
- Cover Letter
- Creative Essay
- Dissertation
- Dissertation - Abstract
- Dissertation - Conclusion
- Dissertation - Discussion
- Dissertation - Hypothesis
- Dissertation - Introduction
- Dissertation - Literature
- Dissertation - Methodology
- Dissertation - Results
- GCSE Coursework
- Grant Proposal
- Marketing Plan
- Multiple Choice Quiz
- Personal Statement
- Power Point Presentation
- Power Point Presentation With Speaker Notes
- Questionnaire
- Reaction Paper
Research Paper
- Research Proposal
- SWOT analysis
- Thesis Paper
- Online Quiz
- Literature Review
- Movie Analysis
- Statistics problem
- Math Problem
- All papers examples
- How It Works
- Money Back Policy
- Terms of Use
- Privacy Policy
- We Are Hiring
Down Syndrome, Research Paper Example
Pages: 5
Words: 1404
Hire a Writer for Custom Research Paper
Use 10% Off Discount: "custom10" in 1 Click 👇
You are free to use it as an inspiration or a source for your own work.
Down syndrome is considered a congenital abnormality whereby the child is born with part of or entirely an additional third copy of the 21 st chromosome combination. Normal people carry 21 distinct pairs of chromosomes. Precise, characteristics of the abnormality are linked to delays in normal growth; peculiar facial features along with mild to moderate intellectual disabilities. Scientists have evaluated the average adult IQ to be 50 -70 related to that of an 8-9 year old child. Other distinct physical features include a small chin; poor muscle tone; slanted eyes; protruding tongue, flat nose; short nose, extra space between first and second toes and a single line in the palms of hands. With modern techniques used in prenatal screening, a diagnostic testing during the second trimester reveals this abnormality and mothers are given a choice of terminating the pregnancy (Roizen & Patterson, 2003).
The epidemiological profile as of 2010 investigations reveals that Down syndrome occurs at a rate of 1 in every 1000 birth globally accounting for an estimated 17,000 deaths annually. Pregnancies occurring at age 40 have a 1 in 84 chance of being Down syndrome. While the incidence of Down syndrome increases with age there is a 30% occurrence among women 35 years of age and under. In 1862, an English physician by the name of John Langdon Down classified the abnormality as specific mental disability (Roizen & Patterson, 2003).
This research relates Down syndrome to Lott Brett book‘s Jewel. Specifics of this novel associated with Down syndrome are contained in the plot. Characters depicted in the plot are Jewel Hilburn, Leston (husband) and their five children. The plot was cited in 1943 when the family was enjoying their best of times in their relationships as well as socially. At age 40 Jewel becomes pregnant with their last child. She was very happy about the development, but became very distressed when her friend predicated that the child would bring harm to the family (Lott, 1999).
At the birth the infant appeared quite normal, but as growth and development stages were observed the family received an astounding diagnosis that the child was ‘ Mongolian idiot’ and would not develop normally. Consequently, the parents were pressured to institutionalize the child they named Brenda Kay. This suggestion was rejected and the family decided to raise this child as normal without medical intervention. At the time there was very little known treatment for this ‘Mongolian idiot’ abnormality now known as Down syndrome. As such, through trial and error Jewel and Leston together raised Brenda Kay accordingly to function as a credible human expression and it was a joy filled experience (Lott, 1999). Essentially, this research project seeks to investigate, what developments in treatment of Downs Syndrome have there been between in the 1950’s and today?
Prior to the Brenda Kay’s birth five healthy children lived in this family. Lott presented this family in a post war era allowing father, Leston, regular employment producing a certain amount of financial prosperity within his family circle. However, with Jewel’s 40 year old pregnancy; birth of a Mongolian idiot child fortunes seemed to have shifted the image of this family within this family. Despite this unfortunate development the Hilburns were committee towards continued prosperity and happiness within their home environment (Lott, 1999).
Subsequently, the family was forced to relocate to California where conditions were different and undue hardships ensued. Amidst these adversity joy flowed as the family enjoyed Brenda Kay company and the eagerness to see how she will develop as a useful human expression. In this new social an geographic environment Jewel develops strategies that will ensure Brenda Kay’s success throughout life. The most effective tools were love and undivided devotion. Immediately she removed from her vocabulary words which did not benefit Brenda’s socialization (Lott, 1999).
They included Mongolian Idiot, as was described by the New Orleans physician, and nigger. During this articulation she discovered the effectiveness of love in treating Down syndrome when there were no scientific remedies for addressing the abnormality. Jewel further described these words as vocabulary that sting. These techniques, perhaps, could be recognized as the first developments in treatment of Down syndrome between 1950 – present time. Due to Jewel’s tenacity and insight the family accomplished its continued prosperity goal in the face of seeming adversity (Lott, 1999).
During the early 20 th century institutionalization was the only treatment for this abnormality. This was primarily due to the fact that the chromosomal element was being disputed and the proposed cause invalidated. Consequently, physiological dysfunctions associated with this disorder were never treated and many children died from the complications of Down syndrome. These included speech impairment; language learning irregularities; heart valve disorders; gastrointestinal disturbances and infertility (Patterson, 2009).
Down syndrome has since emerged into difference phase beginning with prenatal screening and abortion if the mother so desires. Research is ongoing to develop evidence based practices that will address peculiar medical conditions associated with Down syndrome abnormalities. Also, many social programs have developed seeking to integrate Down syndrome people into social as useful citizens. From a medical perspective with the emergence of the eugenics movement laws protecting downs syndrome women from being prosecuted for having abortions was passed in United States of America. Subsequently, 33 of 48 states in United States of America designed legislations forcing sterilization of people with Down syndrome (Patterson, 2009).
Twenty-first century evolutions in Down syndrome medical treatment focus on frequent doctors’ visits evaluating the emergence of predisposing medical conditions directly related to the abnormality. Mental development would be delayed, but children are expected to otherwise enjoy good health obtaining proper nutrition and vaccinations relevant to their age/ weight/height. Common gastrointestinal conditions, which a pediatrician/physician has to be alert in detecting include imperforate anus, esophageal atresia, duodenal atresia or stenosis, tracheoesophageal fistula and Hirschsprung’s disease (Paterson, 2009).
Some infants are born with heart defects such as atrial septal disorder; ventricular septal defect, Fallot’s tetralogy, and patent ductus arteriosus. With modern techniques applied in treatment intervention of Down syndrome beyond institutionalization, frequent doctor’s visits would rule out or confirm any of these associating disorders emerging from the drown syndrome congenital abnormality. Signs and symptoms are further evaluated and specific treatment regimen begins immediately (Paterson, 2009).
Co-existing psychiatric disorders frequently requiring therapeutic intervention include autism spectrum disorders; attention deficit hyperactivity disorder (ADHD), stereotypical movement disorders, depression and obsessive compulsive disorder (OCD). During the 1950’s when Brenda Kay was born and diagnosed a Mongolian idiot no such screening measures were available to Down syndrome children and adults. They were simply ostracized in places designed for living with no hope, love and quality of life until death. Many strides have been made in the treatment science of Down syndrome since 1950s (Paterson, 2009).
For example, musical therapies have been used to improve learning and lengthen the attention span among children with Down syndrome. Studies show where music incorporated in movement help children affected by Down syndrome to synchronize hand eye coordination. It also helped in reducing obesity rates since inactivity makes them susceptible to being overweight. Importantly, the use of music appeared to be soothing and they responded more to the music than the movement regimes they encompassed (Paterson, 2009).
Prior to 1970’s no attempts were made by educational systems, internationally, to include children affected by Own syndrome because they were considered beyond learning capacity. However, with new approaches in special education strategies many children have been given opportunities to develop an education compatible with their IQ and have been self-sufficient. These educational opportunities have allowed people with Down syndrome to participate in the social structure through career pursuits (Paterson, 2009).
Therapeutic riding has also been introduced to influence psychomotor development after Atlantoaxial Instability has been ruled out and the activity would not create further injury if they accidentally fall during the activity. Down syndrome children who have been cleared of this complication respond excellently to horseback riding therapies. Other activities incorporated in therapies are presently being researched with the focus of enhancing the quality of life for people affected by Down syndrome. It is clear that they no longer have to be institutionalized due their perceived uselessness, but rather socialized into becoming. Jewel in Lott’s book did set the pace for down syndrome children/people involvement in the social structure, not as idiots, but unique human beings, who are differently capable.
Works cited
Lott, Brent. Jewels . Washington Square Press. 1999. Print
Patterson, D. Molecular genetic analysis of Down syndrome. Human genetics 126 (1) 2009; 195–214.
Roizen, NJ; Patterson, D. Down’s syndrome. Lancet (Review ) 361 (9365), 2003; 1281–89. Print
Stuck with your Research Paper?
Get in touch with one of our experts for instant help!
Ethical Principles of Psychologists, Essay Example
The Prudent Samaritan, Essay Example
Time is precious
don’t waste it!
Plagiarism-free guarantee
Privacy guarantee
Secure checkout
Money back guarantee

Related Research Paper Samples & Examples
The risk of teenagers smoking, research paper example.
Pages: 11
Words: 3102
Impacts on Patients and Healthcare Workers in Canada, Research Paper Example
Pages: 7
Words: 1839
Death by Neurological Criteria, Research Paper Example
Words: 2028
Ethical Considerations in End-Of-Life Care, Research Paper Example
Words: 1391
Ethical Dilemmas in Brain Death, Research Paper Example
Words: 2005
Politics of Difference and the Case of School Uniforms, Research Paper Example
Pages: 2
Words: 631
MINI REVIEW article
Development of down syndrome research over the last decades–what healthcare and education professionals need to know.

- 1 Division of Obstetrics and Feto-Maternal Medicine, Department of Obstetrics and Gynecology, Medical University of Vienna, Vienna, Austria
- 2 Research Unit Developmental Psychology, Department of Developmental and Educational Psychology, Faculty of Psychology, University of Vienna, Vienna, Austria
Down syndrome (DS) is the most prevalent neurodevelopmental disorder, with a known genetic cause. Besides facial dysmorphologies and congenital and/or acquired medical conditions, the syndrome is characterized by intellectual disability, accelerated aging, and an increased likelihood of an early onset Alzheimer's disease in adulthood. These common patterns of DS are derived from the long-held standard in the field of DS research, that describes individuals with DS as a homogeneous group and compares phenotypic outcomes with either neurotypical controls or other neurodevelopmental disorders. This traditional view has changed, as modern research pinpoints a broad variability in both the occurrence and severity of symptoms across DS, arguing for DS heterogeneity and against a single “DS profile.” Nevertheless, prenatal counseling does not often prioritize the awareness of potential within-group variations of DS, portraying only a vague picture of the developmental outcomes of children with DS to expectant parents. This mini-review provides a concise update on existent information about the heterogeneity of DS from a full-spectrum developmental perspective, within an interdisciplinary context. Knowledge on DS heterogeneity will not only enable professionals to enhance the quality of prenatal counseling, but also help parents to set targeted early interventions, to further optimize daily functions and the quality of life of their children.
Introduction
Down syndrome (DS) is the most common neurodevelopmental disorder with known genetic causes, and an incidence of 1 in 691 live births ( 1 ). This suggests that ~417,000 people with DS live in Europe ( 2 ). Currently, an expansive menu of prenatal diagnostic methods for DS is spreading worldwide, advancing the diagnosis of DS from postnatal to prenatal ( 3 ). Giving an expectant parent a fetal diagnosis of DS provides them with 2 options: keeping or terminating their pregnancy, following the lack of a cure ( 4 ).
Prenatal counseling is crucial for providing parents with an accurate picture of DS so that informed decisions can be made in the context of their own beliefs and values ( 3 ). Although studies are still examining the nature of DS, portraying the expected neurodevelopmental outcomes of affected children remains challenging. Indeed, retrospective studies indicate that parents felt that the information received during prenatal counseling was inaccurate, outdated, and unbalanced, and either too negative or too optimistic ( 5 – 7 ). Without appropriate professional training or updated professional development regarding the individual variability in outcomes associated with DS, prenatal counselors might present expectant parents with inaccurate information or impressions. Therefore, expectant parents may not receive the level of information needed. Accordingly, all professionals working with families affected by DS must be aware of the most current scientific research regarding the heterogeneity of phenotypic outcomes ( 8 ).
This mini-review closes an existent literature gap by providing a concise update on the available information on within-group variations in the DS phenotype of infants, children, and adolescents for professionals. First, a gross outline of DS research is given, focusing on the significant paradigm shift from a group- to an individual-level approach. Second, the current knowledge on significant within-group variations of DS in cognitive, behavioral, emotional, and olfactory functioning is summarized. Finally, the review concludes by arguing that only an interdisciplinary approach allows for the description of realistic individual DS profiles. The scope of this review is to further increase the awareness on DS heterogeneity concerning developmental outcomes.
A Paradigm Shift in DS Research: From a Group- to Individual-Level Approach
DS research dates back to 1866, when the English physician John Langdon Down systematically described the syndrome for the first time ( 9 , 10 ). In addition to intellectual disability (ID), he chronicled a distinct physical phenotype of individuals with DS, conjecturing that they were “born to the same family” (page 9) ( 10 , 11 ). The century following his pioneering work was filled with publications of diverse medical case studies documenting a range of physical traits and medical comorbidities, leading to various etiologies ( 10 , 11 ).
Almost 100 years later, the French pediatrician and cytogeneticist, Jérôme Lejeune, identified the genetic basis of DS in 1959 as an extra copy of all or part of chromosome 21 ( 10 , 12 ). The discovery of “trisomy 21” paved the way for further research, to elucidate genotype-phenotype-relationships ( 13 , 14 ). Since its original description, classical DS research has analyzed the syndrome's phenotypes relative to neurotypicals and/or other neurodevelopmental disorders, hence providing group-level data that have advanced our basic knowledge of DS ( 8 ). It is characterized by both typical physical features that make the syndrome “instantly recognizable” (page 8) and ID ( 11 ). Common appearance includes craniofacial dysmorphologies, short stature, low muscle tone, and a proportionally large tongue. Additionally, medical comorbidities, such as sleep apnea, visual and/or hearing problems, congenital heart defects, and altered behavioral, hematopoietic, endocrine, gastrointestinal, neurological, and musculoskeletal conditions, are linked to DS ( 10 ).
Most of these medical problems are treatable with pharmacotherapy and/or surgical interventions. Therefore, among the key focuses in recent DS research is the widespread field of neurocognition, associating DS with weaknesses in motor ability, auditory processing, verbal short-term memory, and expressive language. However, relative strengths in visuospatial processing, receptive language, and some aspects of social functioning have been reported ( 15 – 18 ). Further, DS is associated with accelerated aging and an increased likelihood of the early onset of Alzheimer's disease (AD) ( 18 ).
Although the generalizability of the characteristics of DS has been questioned repeatedly in the history of DS research, the group-level approach is a long-held standard ( 19 , 20 ). However, this traditional view has changed, following a growing number of studies, which pinpoint significant within-group variations across individuals with DS at many levels of description. Pioneer studies have launched this paradigm shift, from a group to an individual-level approach, by highlighting significant individual differences in genetics, cell biology, brain research, and subsequently, parts of cognitive research on DS [see ( 8 )]. These studies suggest that this heterogeneity may be continued in DS phenotypes ( 8 ). The following review aims to supplement the prevailing knowledge about the variability of the developmental outcomes of DS by addressing this issue from an interdisciplinary and applied science perspective, as this practical information may be the most useful for professionals to pass to expectant parents.
Infants, Children, and Adolescents With DS: Variability in Developmental Outcomes
Acquisition of developmental milestones.
Generally, it was assumed that infants and children with DS reached developmental milestones in the same linear fashion as their non-DS peers, but at later chronological ages. This view is too simplistic, as the age of acquiring milestones among infants and children with DS is reported to vary significantly ( 21 , 22 ). For example, the mean age at the onset of babbling is ~15 months, with an interindividual variability of 10 months. Similarly, sphincter control is acquired by DS children at an approximate age of 44 months, with 22 months of interindividual variability ( 22 ). Notably, Locatelli et al. suggested that the age at which developmental milestones are reached influences the subsequent development of diverse cognitive domains significantly ( 21 , 22 ).
Intellectual Disability (ID)
ID, defined by an intelligence quotient (IQ) score of <70, is reported to be universal in the DS population. However, this construct presents in DS with large interindividual variability ( 23 ). The majority of individuals with DS fall within the severe (IQ 20–35) to mild (IQ 50–69) range of ID. However, some cases reach IQ scores equivalent to children without ID ( 14 , 24 ). Research on the developmental trajectories of cognitive function in neurotypicals shows that IQ is a construct that remains relatively stable and consistent across ages. A slight decline was observed only in older adults ( 14 ). Conversely, DS research has identified a linear decline in IQ scores as development progresses, starting in the first year of life (i.e., cognitive gains do not keep pace with chronological age). Notably, single IQ levels and the degree of cognitive decline vary across the DS group ( 14 ).
Language is another cognitive domain that generates significant differences among individuals with DS. DS is associated with weaknesses in expressive language and a relative strength in the receptive language ( 18 ). The available literature reports developmental delays in both language domains, becoming apparent no later than age five, yet with wide individual differences ( 25 , 26 ). Regarding vocabulary acquisition and growth, longitudinal studies reported an existing continuum, ranging from non-verbal children to those with a vocabulary close to the normal range ( 27 , 28 ). Children with DS use gestures as a means of communication, which has been positively associated with the development of spoken vocabulary ( 29 ). Nevertheless, significant individual variability in the extent to which this “gestural advantage” is used has been demonstrated by empirical data ( 30 ). All within-group differences in language development persist into adulthood ( 26 ).
Memory and learning deficits are universal characteristics of DS and are known to become more pronounced as development progresses ( 14 ). In classical DS research, the findings of affected memory domains are mixed, suggesting underlying variability ( 18 ). Indeed, scientific data demonstrate that there are individual differences in both implicit and explicit memory ( 8 , 31 ). Regarding the latter, significant within-group variations are described for short-term verbal and long-term visual memory ( 8 ). Individuals with DS often show deficits in processing local detail. Therefore, classical DS literature claims that individuals with DS were “global processors.” However, this preference for global over local processing does not always occur in the DS population. Therefore, individuals with DS cannot be simply categorized into one of these processing styles ( 32 ).
Executive Function (EF)
EF encompasses a range of cognitive processes involved in goal-oriented behavior, and is a domain in which individuals with DS are shown to have pronounced difficulties ( 33 ). The areas of working memory, attention, planning, and inhibition are considered particularly challenging for individuals with DS; emotional control is considered a relative strength ( 34 , 35 ). However, significant individual differences in EF across the DS group have become evident ( 33 , 36 ). Within-group variations in auditory attention have been identified via electrophysiological measurement among toddlers with DS, data that also predict differences in language abilities as development progresses ( 37 ). Patterns of executive dysfunction appear to be relatively consistent across development until adulthood ( 23 , 34 ).
Adaptive Behavior (AB)
Children and adolescents with DS are known to be severely impaired in AB, which subsumes behavioral skills that enable them to function independently in their everyday life ( 23 , 38 ). Generally, AB encompasses 4 domains: socialization, communication, daily living, and motor skills ( 23 ). Significant within-group variations were apparent for all the 4 domains. For example, DS has been associated with sociability, friendliness, affection, empathy, good competence in forming relationships, and high tendency to smile ( 39 ). Yet, children and adolescents with DS are also considered stubborn, to show little accommodation to social partners, and approach strangers inappropriately ( 40 ). Some individuals with DS have even deficits in socialization to the extent of a comorbid diagnosis of autism ( 41 ).
Maladaptive Behavior (MB) and Psychiatric Comorbidities
MB encompasses a range of behaviors that impede an individual's activities of daily living or the ability to adjust to and participate in particular settings ( 23 ). Approximately 1/4 to 1/3 of individuals with DS exhibit clinically significant levels of maladaptive behavioral concerns ( 42 – 44 ). This behavioral construct is another domain that yields significant within-group differences ( 21 , 23 , 45 ). More difficulties with “anxious-depressed” symptoms are observed among adolescents than younger children with DS ( 23 ). Children with DS often exhibit externalizing behavior ( 46 ). The manifestation of MB is significantly higher when neurobehavioral disorders are concomitant ( 47 – 49 ). According to the available literature, the manifestation of psychiatric features, including autism, depression, and the attention-deficit/hyperactivity disorder, vary significantly, between 6 and >50% ( 42 , 44 , 50 , 51 ). Channell et al. underscored within-group differences in the behavioral domain by subtyping a >300-person DS group, hence identifying a separate “behavioral” class as described in Table 1 ( 23 ).

Table 1 . Characterization of the 3-class model of individuals with DS ( N = 314; 6–25 years) based on the variability observed in cognitive and behavioral measures, identified by Channell et al. ( 23 ) using a latent profile analysis.
Emotional Functioning
The emotional profiles of individuals with DS have remained underexplored, which could be attributed to the assumed stereotype of high sociability in this population ( 52 , 53 ). Available literature provides variable data about whether children and adolescents have difficulties in emotional functioning ( 52 ). Whereas, some studies negate differences in identifying basic emotion in faces between DS and non-DS groups, other scientific reports indicate that children and adolescents with DS have impairments in this emotional skill [see Roch et al. ( 52 )] ( 54 – 57 ). Deficits in recognizing facial expressions were not generalized to all emotions, but mostly to fear ( 52 , 58 ). Other studies report impairments in determining feelings, including surprise, anger, and neutral expression ( 40 , 58 – 61 ). Some studies pinpoint problems in ascertaining negative emotions ( 40 ). Moreover, an inability to distinguish between fear and sadness is another atypical pattern that has been reported among some individuals ( 58 ). Most of these deficits are identified during infancy and childhood. Therefore, a negative impact on the subsequent development of interpersonal relationships is discussed ( 52 ). As previously mentioned, studies have exclusively gathered data at the group level. Moreover, further research should examine whether inconsistencies in findings across studies can be attributed to underlying within-group variations.
Olfactory Functioning
The number of studies on olfactory function among patients with DS is limited and relatively out of date ( 62 – 69 ). Historical studies have described olfactory deficits in the DS population for many years ( 62 , 63 , 65 , 70 ). Because rhinologic pathologies have been ruled out by studies showing nasal function in DS as comparable to controls, central-nervous causes are suggested ( 64 ). More recently, Cecchini et al. described olfactory function as severely impaired among adults with DS ( 71 ). They found a positive correlation between odor identification and cognition ( 71 ). To date, the largest study, which included people with DS and under 18 years, described a minimal impairment of olfactory functioning among children and adolescents (9–17 years), which became pronounced in young adulthood (18–29 years) and was the lowest in adulthood (30–50 years) ( 72 ). Of the three groups, DS, IQ, and age-matched controls, significant within-group differences were evident only in the DS group ( 72 ). However, large and detailed analyses of olfactory function in light of within-group variations among children and adolescents with DS are still lacking. Odor identification deficits are considered a valid non-invasive early marker of AD. Therefore, future research on whether olfactory dysfunction can help to ascertain the subset of children and adolescents with DS that will later develop AD is warranted.
Alzheimer's Disease (AD)
Although the issue of AD appears outside the scope of this review, the following considerations must be made when the heterogeneity of DS is discussed with expectant parents from a full-spectrum developmental perspective. Owing to a shared genetic predisposition, individuals with DS have an increased likelihood of developing early onset AD in adulthood ( 18 ). Prevalence rates of dementia among the DS population vary significantly in the literature, from 8 to 100% ( 18 , 73 ). Recent brain research has identified Alzheimer's plaques among some children with DS, that is, as early as 8 years of age, whereas some DS brains show no plaques until early adulthood ( 14 , 26 ). Although AD neuropathology occurs in virtually all individuals with DS over the age of 30, only a subset of people develop clinical symptoms of dementia ( 26 , 74 , 75 ). Hence, it is apparent that the widespread interindividual variability, typical for DS, is a pivotal feature not only during development, but also during aging ( 26 ). Aging is part of the continuous lifespan development. Accordingly, some authors argue that AD should be considered a disease that occurs during development, rather than aging ( 76 ).
Extrinsic Influencing Factors of Developmental Outcomes of Infants, Children, and Adolescents With DS
Medical comorbidities.
In addition to cognitive limitations, parents must be informed that there is a list of medical comorbidities associated with DS. Some of them, including congenital heart defects (CHD), seizures, visual and/or hearing impairments, autism, and sleep disruptions, are known to moderate cognitive functioning ( 18 ). Analogous to neurodevelopmental outcomes, both the occurrence and expression of congenital and/or acquired medical complications are variable ( 18 ). For example, 41–56% of infants with DS are born with a CHD, with an atrioventricular septal defect that occurs between 31 and 61% being the most common form ( 77 , 78 ). Cognition, gross motor skills, and language are significantly worse among infants with DS and CHD, relative to peers without CHD, in some, but not in all related studies ( 79 – 81 ). For example, Alsaied et al. showed that children with DS and CHD, who undergo cardiac surgery during their first year, have no significant differences in neurodevelopmental outcomes at preschool and school age. However, as infants and toddlers, they were prone to poorer outcomes in receptive, expressive, and composite language compared to children with DS without CHD, suggesting that deleterious effects may be dependent on clinical management ( 82 ).
Home Environment
Another variable that affects the observed variability of DS phenotypes, which is influenced by the expectant parents, is the home environment. According to Karmiloff-Smith et al., the genetic syndrome changes the family context in terms of parent-child-interactions ( 8 ). D'Souza et al. demonstrated that parental depression, a disease linked to difficulties in responding to the child in a sensitive and consistent manner, explained deficits in expressive language development among children between 8 and 48 months of age with DS ( 83 ). Similarly, there is evidence that vocabulary development among children with DS is influenced by how parents respond to their children's communication. Deckers et al. argued that mothers with a higher level of education had a better ability to fine-tune their communication with their children with DS ( 28 ). Further demographic factors, including socioeconomic status, neighborhood demographics, and the availability of therapeutic resources, modulate the developmental outcomes of DS effectively ( 84 , 85 ). These data demonstrate that only an interdisciplinary approach that considers psychological, physical, and social parameters will enable professionals to accurately inform expectant parents on how the DS phenotype will be expressed in each individual.
Although DS has been examined for a long time, that is 155 years, it is still one of the least understood genetic ID syndromes. The most significant reason for this is the high degree of phenotypic variability observed in the DS population, an issue that professionals are often unaware of when discussing the diagnosis with expectant parents. However, DS research has advanced from a group to an individual-level approach, attempting to acknowledge within-group differences at many levels of basic science ( 8 ). To expand on this wealth of data, this mini-review has shed light on the available information on individual variability in the developmental outcomes of infants, children, and adolescents with DS from an applied science perspective, which will enhance the quality of prenatal counseling. Diverse developmental domains, including cognition, behavior, and emotional and olfactory functioning, have been discussed.
The evaluation of developmental outcomes from a full-spectrum perspective, however, must not only address different developmental domains, but also the change of phenotypes over time ( 86 ). Outcome variables are not completely intact or impaired uniformly throughout development, but manifest as variations at an early state, that may be magnified with age, ending up as either a strength or a weakness. Therefore, parents should be made aware that early development can be considered a critical window of opportunity to set adequate phenotype-specific interventions before deficits become severely pronounced ( 87 ). Thus, the maximization of individual potential is possible. In addition to psychological factors, other influencing variables must be considered by parents when the variability of DS phenotypes is discussed. According to Karmiloff-Smith who states that having a neurodevelopmental disorder changes both the social environment and physical status, only an interdisciplinary research approach can successfully describe valid profiles of individuals with DS ( 8 ).
The most convincing argument for emphasizing individual variability among DS groups and discussing them with expectant parents are both an average life expectancy of 60 years combined with an early onset of Alzheimer's disease in the DS population ( 18 ). Focusing on individual differences in the development of DS may be the best approach for exploring the risk and protective factors of AD ( 88 , 89 ).
Modern DS research shows that developmental heterogeneity has become increasingly validated ( 23 ). Moving forward, these up-to-date data must be disseminated under the supervision of professionals so that prenatal counseling can be optimized in quality, hence allowing parents to gain realistic expectations about the future of their children. Thus, more targeted treatments and interventions can be set to improve the daily function and quality of life.
Author Contributions
KW and SH designed the paper. KW did the literature research and wrote the manuscript. SH provided intellectual input and critically revised the manuscript. Both authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. (2010) 88:1008–16. doi: 10.1002/bdra.20735
PubMed Abstract | CrossRef Full Text | Google Scholar
2. de Graaf G, Buckley F, Skotko BG. Estimation of the number of people with Down syndrome in Europe. Eur J Hum Genet. (2021) 29:402–10. doi: 10.1038/s41431-020-00748-y
3. Minear MA, Alessi S, Allyse M, Michie M, Chandrasekharan S. Noninvasive prenatal genetic testing: current and emerging ethical, legal, and social issues. Annu Rev Genomics Hum Genet. (2015) 16:369–98. doi: 10.1146/annurev-genom-090314-050000
4. Guedj F, Bianchi DW. Noninvasive prenatal testing creates an opportunity for antenatal treatment of Down syndrome. Prenat Diagn. (2013) 33:614–8. doi: 10.1002/pd.4134
5. Skotko BG, Kishnani PS, Capone GT, Group DSDS. Prenatal diagnosis of Down syndrome: how best to deliver the news. Am J Med Genet A . (2009) 149A:2361–7. doi: 10.1002/ajmg.a.33082
6. Zerres K, Rudnik-Schöneborn S, Holzgreve W. Do non-invasive prenatal tests promote discrimination against people with Down syndrome? What should be done? J Perinat Med. (2021) 49:965–71. doi: 10.1515/jpm-2021-0204
7. Skotko BG. With new prenatal testing, will babies with Down syndrome slowly disappear? Arch Dis Child. (2009) 94:823–6. doi: 10.1136/adc.2009.166017
8. Karmiloff-Smith A, Al-Janabi T, D'Souza H, Groet J, Massand E, Mok K, et al. The importance of understanding individual differences in Down syndrome. F1000Res . (2016) 5:389. doi: 10.12688/f1000research.7506.1
9. Down JL. Observations on an ethnic classification of idiots. Ment Retard . (1995) 33:54–6.
Google Scholar
10. Hickey F, Hickey E, Summar KL. Medical update for children with Down syndrome for the pediatrician and family practitioner. Adv Pediatr. (2012) 59:137–57. doi: 10.1016/j.yapd.2012.04.006
11. D W. Downs: The History of a Disability. Oxford: Oxford University Press (2011).
12. Lejeune J, Gautier M, Turpin R. Study of somatic chromosomes from 9 mongoloid children. C R Hebd Seances Acad Sci. (1959) 248:1721–2.
PubMed Abstract | Google Scholar
13. Patterson D, Costa AC. Down syndrome and genetics - a case of linked histories. Nat Rev Genet. (2005) 6:137–47. doi: 10.1038/nrg1525
14. Lukowski AF, Milojevich HM, Eales L. Cognitive functioning in children with down syndrome: current knowledge and future directions. Adv Child Dev Behav. (2019) 56:257–89. doi: 10.1016/bs.acdb.2019.01.002
15. Daunhauer LA, Fidler DJ. The down syndrome behavioral phenotype: implications for practice and research in occupational therapy. Occup Ther Health Care. (2011) 25:7–25. doi: 10.3109/07380577.2010.535601
16. Jarrold C, Baddeley AD. Short-term memory for verbal and visuospatial information in down's syndrome. Cogn Neuropsychiatry. (1997) 2:101–22. doi: 10.1080/135468097396351
17. Jarrold C, Baddeley AD, Phillips C. Down syndrome and the phonological loop: the evidence for, and importance of, a specific verbal short-term memory deficit. Downs Syndr Res Pract. (1999) 6:61–75. doi: 10.3104/reviews.97
18. Grieco J, Pulsifer M, Seligsohn K, Skotko B, Schwartz A. Down syndrome: cognitive and behavioral functioning across the lifespan. Am J Med Genet C Semin Med Genet. (2015) 169:135–49. doi: 10.1002/ajmg.c.31439
19. Desai SS. Down syndrome: a review of the literature. Oral Surg Oral Med Oral. (1997) 84:279–85. doi: 10.1016/S1079-2104(97)90343-7
20. Hodapp RM. Studying interactions, reactions, and perceptions: can genetic disorders serve as behavioral proxies? J Autism Dev Disord. (2004) 34:29–34. doi: 10.1023/B:JADD.0000018071.02942.00
21. van Gameren-Oosterom HB, Fekkes M, Buitendijk SE, Mohangoo AD, Bruil J, Van Wouwe JP. Development, problem behavior, and quality of life in a population based sample of eight-year-old children with Down syndrome. PLoS ONE. (2011) 6:e21879. doi: 10.1371/journal.pone.0021879
22. Locatelli C, Onnivello S, Antonaros F, Feliciello A, Filoni S, Rossi S, et al. Is the age of developmental milestones a predictor for future development in down syndrome? Brain Sci. (2021) 11:655. doi: 10.3390/brainsci11050655
23. Channell MM, Mattie LJ, Hamilton DR, Capone GT, Mahone EM, Sherman SL, et al. Capturing cognitive and behavioral variability among individuals with Down syndrome: a latent profile analysis. J Neurodev Disord. (2021) 13:16. doi: 10.1186/s11689-021-09365-2
24. Edgin JO. Cognition in Down syndrome: a developmental cognitive neuroscience perspective. Wiley Interdiscip Rev Cogn Sci. (2013) 4:307–17. doi: 10.1002/wcs.1221
25. Guralnick MJ. Involvement with peers: comparisons between young children with and without Down's syndrome. J Intellect Disabil Res. (2002) 46(Pt5):379–93. doi: 10.1046/j.1365-2788.2002.00405.x
26. Thomas MSC, Ojinaga Alfageme O, D'Souza H, Patkee PA, Rutherford MA, Mok KY, et al. A multi-level developmental approach to exploring individual differences in Down syndrome: genes, brain, behaviour, and environment. Res Dev Disabil. (2020) 104:103638. doi: 10.1016/j.ridd.2020.103638
27. Zampini L, D'Odorico L. Communicative gestures and vocabulary development in 36-month-old children with Down's syndrome. Int J Lang Commun Disord. (2009) 44:1063–73. doi: 10.1080/13682820802398288
28. Deckers SRJM, Van Zaalen Y, Van Balkom H, Verhoeven L. Predictors of receptive and expressive vocabulary development in children with Down syndrome. Int J Speech Lang Pathol. (2019) 21:10–22. doi: 10.1080/17549507.2017.1363290
29. Özçalişkan S, Adamson LB, Dimitrova N, Baumann S. Early gesture provides a helping hand to spoken vocabulary development for children with autism, Down syndrome and typical development. J Cogn Dev. (2017) 18:325–37. doi: 10.1080/15248372.2017.1329735
30. Kaat-van den Os D, Volman C, Jongmans M, Lauteslager P. Expressive vocabulary development in children with down syndrome: a longitudinal study. J Policy Pract Intellect Disabil. (2016) 14:311–8. doi: 10.1111/jppi.12212
CrossRef Full Text | Google Scholar
31. Vicari S. Implicit versus explicit memory function in children with Down and Williams syndrome. Downs Syndr Res Pract. (2001) 7:35–40. doi: 10.3104/reports.112
32. D'Souza D, Booth R, Connolly M, Happé F, Karmiloff-Smith A. Rethinking the concepts of 'local or global processors': evidence from Williams syndrome, Down syndrome, and Autism Spectrum Disorders. Dev Sci. (2016) 19:452–68. doi: 10.1111/desc.12312
33. Tungate AS, Conners FA. Executive function in Down syndrome: a meta-analysis. Res Dev Disabil. (2021) 108:103802. doi: 10.1016/j.ridd.2020.103802
34. Loveall SJ, Conners FA, Tungate AS, Hahn LJ, Osso TD. A cross-sectional analysis of executive function in Down syndrome from 2 to 35 years. J Intellect Disabil Res. (2017) 61:877–87. doi: 10.1111/jir.12396
35. Lee NR, Anand P, Will E, Adeyemi EI, Clasen LS, Blumenthal JD, et al. Everyday executive functions in Down syndrome from early childhood to young adulthood: evidence for both unique and shared characteristics compared to youth with sex chromosome trisomy (XXX and XXY). Front Behav Neurosci. (2015) 9:264. doi: 10.3389/fnbeh.2015.00264
36. Grealish KG, Price AM, Stein DS. Systematic review of recent pediatric down syndrome neuropsychology literature: considerations for regression assessment and monitoring. J Dev Behav Pediatr. (2020) 41:486–95. doi: 10.1097/DBP.0000000000000800
37. D'Souza D, D'Souza H, Johnson MH, Gliga T, Kushnerenko E, Scerif G, et al. Are early neurophysiological markers of ASD syndrome-specific? A cross-syndrome comparison. In: Paper presented at the XIX Biennial International Conference on Infant Studies. Berlin: International Society on Infant Studies (2014).
38. de Weger C, Boonstra FN, Goossens J. Differences between children with Down syndrome and typically developing children in adaptive behaviour, executive functions and visual acuity. Sci Rep. (2021) 11:7602. doi: 10.1038/s41598-021-85037-4
39. Fidler DJ. The emerging Down syndrome behavioral phenotype in early childhood. Infants Young Child. (2005) 18:86–103. doi: 10.1097/00001163-200504000-00003
40. Porter MA, Coltheart M, Langdon R. The neuropsychological basis of hypersociability in Williams and Down syndrome. Neuropsychologia. (2007) 45:2839–49. doi: 10.1016/j.neuropsychologia.2007.05.006
41. Glennon JM, Karmiloff-Smith A, Thomas MSC. Syndromic autism: progressing beyond current levels of description. Rev J Autism Dev Disord. (2017) 4:321–7. doi: 10.1007/s40489-017-0116-2
42. Dykens EM. Psychiatric and behavioral disorders in persons with Down syndrome. Ment Retard Dev Disabil Res Rev. (2007) 13:272–8. doi: 10.1002/mrdd.20159
43. Coe DA, Matson JL, Russell DW, Slifer KJ, Capone GT, Baglio C, et al. Behavior problems of children with Down syndrome and life events. J Autism Dev Disord. (1999) 29:149–56. doi: 10.1023/A:1023044711293
44. Roizen NJ, Patterson D. Down's syndrome. Lancet. (2003) 361:1281–9. doi: 10.1016/S0140-6736(03)12987-X
45. van Gameren-Oosterom HB, Fekkes M, van Wouwe JP, Detmar SB, Oudesluys-Murphy AM, Verkerk PH. Problem behavior of individuals with Down syndrome in a nationwide cohort assessed in late adolescence. J Pediatr. (2013) 163:1396–401. doi: 10.1016/j.jpeds.2013.06.054
46. Dykens EM, Shah B, Sagun J, Beck T, King BH. Maladaptive behaviour in children and adolescents with Down's syndrome. J Intellect Disabil Res. (2002) 46(Pt6):484–92. doi: 10.1046/j.1365-2788.2002.00431.x
47. Capone GT, Grados MA, Kaufmann WE, Bernad-Ripoll S, Jewell A. Down syndrome and comorbid autism-spectrum disorder: characterization using the aberrant behavior checklist. Am J Med Genet A. (2005) 134:373–80. doi: 10.1002/ajmg.a.30622
48. Carter JC, Capone GT, Gray RM, Cox CS, Kaufmann WE. Autistic-spectrum disorders in Down syndrome: further delineation and distinction from other behavioral abnormalities. Am J Med Genet B Neuropsychiatr Genet. (2007) 144B:87–94. doi: 10.1002/ajmg.b.30407
49. Ji NY, Capone GT, Kaufmann WE. Autism spectrum disorder in Down syndrome: cluster analysis of Aberrant Behaviour Checklist data supports diagnosis. J Intellect Disabil Res. (2011) 55:1064–77. doi: 10.1111/j.1365-2788.2011.01465.x
50. Siegel MS, Smith WE. Psychiatric features in children with genetic syndromes: toward functional phenotypes. Pediatr Clin North Am. (2011) 58:833–64. doi: 10.1016/j.pcl.2011.06.010
51. Capone G, Goyal P, Ares W, Lannigan E. Neurobehavioral disorders in children, adolescents, and young adults with Down syndrome. Am J Med Genet C Semin Med Genet. (2006) 142C:158–72. doi: 10.1002/ajmg.c.30097
52. Roch M, Pesciarelli F, Leo I. How individuals with down syndrome process faces and words conveying emotions? Evidence From a Priming Paradigm. Front Psychol. (2020) 11:692. doi: 10.3389/fpsyg.2020.00692
53. Pitcairn TK, Wishart JG. Reactions of young children with Down's syndrome to an impossible task. Br J Dev Psychol. (1994) 12:485–9. doi: 10.1111/j.2044-835X.1994.tb00649
54. Turk J, Cornish K. Face recognition and emotion perception in boys with fragile-X syndrome. J Intellect Disabil Res. (1998) 42:490–9. doi: 10.1046/j.1365-2788.1998.4260490.x
55. Celani G, Battacchi MW, Arcidiacono L. The understanding of the emotional meaning of facial expressions in people with autism. J Autism Dev Disord. (1999) 29:57–66. doi: 10.1023/A:1025970600181
56. Goldman KJ, Shulman C, Bar-Haim Y, Abend R, Burack JA. Attention allocation to facial expressions of emotion among persons with Williams and Down syndromes. Dev Psychopathol. (2017) 29:1189–97. doi: 10.1017/S0954579416001231
57. Martínez-Castilla P, Burt M, Borgatti R, Gagliardi C. Facial emotion recognition in Williams syndrome and Down syndrome: a matching and developmental study. Child Neuropsychol. (2015) 21:668–92. doi: 10.1080/09297049.2014.945408
58. Wishart JG, Cebula KR, Willis DS, Pitcairn TK. Understanding of facial expressions of emotion by children with intellectual disabilities of differing aetiology. J Intellect Disabil Res. (2007) 51(Pt7):551–63. doi: 10.1111/j.1365-2788.2006.00947.x
59. Hippolyte L, Barisnikov K, Van der Linden M. Face processing and facial emotion recognition in adults with Down syndrome. Am J Ment Retard. (2008) 113:292–306. doi: 10.1352/0895-8017(2008)113[292:FPAFER]2.0.CO;2
60. Kasari C, Freeman SF, Hughes MA. Emotion recognition by children with Down syndrome. Am J Ment Retard. (2001) 106:59–72. doi: 10.1352/0895-8017(2001)106<0059:ERBCWD>2.0.CO;2
61. Wishart JG, Pitcairn TK. Recognition of identity and expression in faces by children with Down syndrome. Am J Ment Retard. (2000) 105:466–79. doi: 10.1352/0895-8017(2000)105 <0466:ROIAEI>2.0.CO;2
62. Murphy C, Jinich S. Olfactory dysfunction in Down's Syndrome. Neurobiol Aging. (1996) 17:631–7. doi: 10.1016/0197-4580(96)00008-5
63. Hemdal P, Corwin J, Oster H. Olfactory identification deficits in Down's syndrome and idiopathic mental retardation. Neuropsychologia. (1993) 31:977–84. doi: 10.1016/0028-3932(93)90152-P
64. Chen MA, Lander TR, Murphy C. Nasal health in Down syndrome: a cross-sectional study. Otolaryngol Head Neck Surg. (2006) 134:741–5. doi: 10.1016/j.otohns.2005.12.035
65. Warner MD, Peabody CA, Berger PA. Olfactory deficits and Down's syndrome. Biol Psychiatry. (1988) 23:836–9. doi: 10.1016/0006-3223(88)90073-X
66. Zucco GM, Negrin NS. Olfactory deficits in Down subjects: a link with Alzheimer disease. Percept Mot Skills. (1994) 78:627–31. doi: 10.2466/pms.1994.78.2.627
67. McKeown DA, Doty RL, Perl DP, Frye RE, Simms I, Mester A. Olfactory function in young adolescents with Down's syndrome. J Neurol Neurosurg Psychiatry. (1996) 61:412–4. doi: 10.1136/jnnp.61.4.412
68. Wetter S, Murphy C. Individuals with Down's syndrome demonstrate abnormal olfactory event-related potentials. Clin Neurophysiol. (1999) 110:1563–9. doi: 10.1016/S1388-2457(99)00086-3
69. Sliger M, Lander T, Murphy C. Effects of the ApoE epsilon4 allele on olfactory function in Down syndrome. J Alzheimers Dis. (2004) 6:397–402; discussion 43–9. doi: 10.3233/JAD-2004-6407
70. Brousseau K, Brainerd MG. A Study of the Physical and Mental Characteristics of Mongoloid Imbeciles. Baltimore: Williams and Wilkins (1928). doi: 10.1097/00000441-192808000-00020
71. Cecchini MP, Viviani D, Sandri M, Hähner A, Hummel T, Zancanaro C. Olfaction in people with down syndrome: a comprehensive assessment across four decades of age. PLoS ONE. (2016) 11:e0146486. doi: 10.1371/journal.pone.0146486
72. Nijjar RK, Murphy C. Olfactory impairment increases as a function of age in persons with Down syndrome. Neurobiol Aging. (2002) 23:65–73. doi: 10.1016/S0197-4580(01)00263-9
73. Zigman WB, Lott IT. Alzheimer's disease in Down syndrome: neurobiology and risk. Ment Retard Dev Disabil Res Rev. (2007) 13:237–46. doi: 10.1002/mrdd.20163
74. Head E, Silverman W, Patterson D, Lott IT. Aging and down syndrome. Curr Gerontol Geriatr Res. (2012) 2012:412536. doi: 10.1155/2012/412536
75. Head E, Powell D, Gold BT, Schmitt FA. Alzheimer's disease in down syndrome. Eur J Neurodegener Dis. (2012) 1:353–64.
76. Karmiloff-Smith A. What Can Studying Babies With Down Syndrome Possibly Tell Us About Alzheimer's Disease in Adults? UCSD Dart Neuroscience Seminar. Retrieved from: https://tdlcucsdedu/research/DNS/videos/Karmiloff-Smithmp4 (accessed August 28, 2019).
77. Torfs CP, Christianson RE. Anomalies in Down syndrome individuals in a large population-based registry. Am J Med Genet. (1998) 77:431–8. doi: 10.1002/(SICI)1096-8628(19980605)77:5<431::AID-AJMG15>3.0.CO;2-J
78. Freeman SB, Bean LH, Allen EG, Tinker SW, Locke AE, Druschel C, et al. Ethnicity, sex, and the incidence of congenital heart defects: a report from the National Down Syndrome Project. Genet Med. (2008) 10:173–80. doi: 10.1097/GIM.0b013e3181634867
79. Visootsak J, Mahle WT, Kirshbom PM, Huddleston L, Caron-Besch M, Ransom A, et al. Neurodevelopmental outcomes in children with Down syndrome and congenital heart defects. Am J Med Genet A. (2011) 155A:2688–91. doi: 10.1002/ajmg.a.34252
80. Visootsak J, Huddleston L, Buterbaugh A, Perkins A, Sherman S, Hunter J. Influence of CHDs on psycho-social and neurodevelopmental outcomes in children with Down syndrome. Cardiol Young. (2016) 26:250–6. doi: 10.1017/S1047951115000062
81. Startin CM, D'Souza H, Ball G, Hamburg S, Hithersay R, Hughes KMO, et al. Health comorbidities and cognitive abilities across the lifespan in Down syndrome. J Neurodev Disord. (2020) 12:4. doi: 10.1186/s11689-019-9306-9
82. Alsaied T, Marino BS, Esbensen AJ, Anixt JS, Epstein JN, Cnota JF. Does congenital heart disease affect neurodevelopmental outcomes in children with down syndrome? Congenit Heart Dis. (2016) 11:26–33. doi: 10.1111/chd.12322
83. D'Souza H, Lathan A, Karmiloff-Smith A, Mareschal D. Down syndrome and parental depression: A double hit on early expressive language development. Res Dev Disabil. (2020) 100:103613. doi: 10.1016/j.ridd.2020.103613
84. Cebula KR, Moore DG, Wishart JG. Social cognition in children with Down's syndrome: challenges to research and theory building. J Intellect Disabil Res. (2010) 54:113–34. doi: 10.1111/j.1365-2788.2009.01215.x
85. Moore DG, Oates JM, Hobson RP, Goodwin J. Cognitive and social factors in the development of infants with Down syndrome. Downs Syndr Res Pract. (2002) 8:43–52. doi: 10.3104/reviews.129
86. Karmiloff-Smith A, Grant J, Berthoud I, Davies M, Howlin P, Udwin O. Language and Williams syndrome: how intact is “intact”? Child Dev. (1997) 68:246–62. doi: 10.1111/j.1467-8624.1997.tb01938.x
87. Karmiloff-Smith A. Development itself is the key to understanding developmental disorders. Trends Cogn Sci. (1998) 2:389–98. doi: 10.1016/S1364-6613(98)01230-3
88. Lott IT, Head E. Dementia in Down syndrome: unique insights for Alzheimer disease research. Nat Rev Neurol. (2019) 15:135–47. doi: 10.1038/s41582-018-0132-6
89. Hithersay R, Startin CM, Hamburg S, Mok KY, Hardy J, Fisher EMC, et al. Association of Dementia With Mortality Among Adults With Down Syndrome Older Than 35 Years. JAMA Neurol. (2019) 76:152–60. doi: 10.1001/jamaneurol.2018.3616
Keywords: Down syndrome, trisomy 21, developmental outcome, phenotypic heterogeneity, Alzheimer's disease, medical comorbidities, social environment, prenatal counseling
Citation: Windsperger K and Hoehl S (2021) Development of Down Syndrome Research Over the Last Decades–What Healthcare and Education Professionals Need to Know. Front. Psychiatry 12:749046. doi: 10.3389/fpsyt.2021.749046
Received: 28 July 2021; Accepted: 22 November 2021; Published: 14 December 2021.
Reviewed by:
Copyright © 2021 Windsperger and Hoehl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefanie Hoehl, stefanie.hoehl@univie.ac.at
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Phenotyping Down syndrome: discovery and predictive modelling with electronic medical records

Apr 22, 2024, 2:52 AM
Nguyen, T. Q., Kerley, C. I., Key, A. P., Maxwell-Horn, A. C., Wells, Q. S., Neul, J. L., Cutting, L. E., & Landman, B. A. (2024). Phenotyping Down syndrome: discovery and predictive modelling with electronic medical records. Journal of Intellectual Disability Research. https://doi.org/10.1111/JIR.13124
A comprehensive two-part study utilizing electronic medical records from Vanderbilt University Medical Center investigated health conditions in individuals with Down syndrome (DS), particularly those with congenital heart disease (CHD). The first part of the study examined a large cohort of DS individuals, revealing a higher prevalence of specific health issues such as heart failure, pulmonary heart disease, and hypothyroidism compared to controls and those with other intellectual and developmental disabilities. The second part focused on DS patients with CHD, identifying conditions like congestive heart failure and valvular heart disease that increased the likelihood of surgical interventions. These findings highlight the complex health profiles of individuals with DS, suggesting the need for tailored medical approaches to better manage their multiple health challenges.
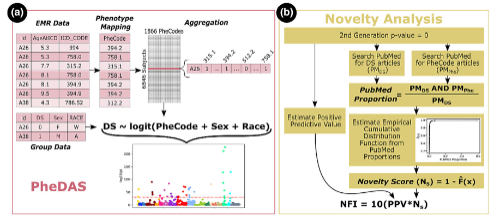
Explore Story Topics
- development
- electronic health records
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 06 May 2024
APOE4 homozygozity represents a distinct genetic form of Alzheimer’s disease
- Juan Fortea ORCID: orcid.org/0000-0002-1340-638X 1 , 2 , 3 na1 ,
- Jordi Pegueroles ORCID: orcid.org/0000-0002-3554-2446 1 , 2 ,
- Daniel Alcolea ORCID: orcid.org/0000-0002-3819-3245 1 , 2 ,
- Olivia Belbin ORCID: orcid.org/0000-0002-6109-6371 1 , 2 ,
- Oriol Dols-Icardo ORCID: orcid.org/0000-0003-2656-8748 1 , 2 ,
- Lídia Vaqué-Alcázar 1 , 4 ,
- Laura Videla ORCID: orcid.org/0000-0002-9748-8465 1 , 2 , 3 ,
- Juan Domingo Gispert 5 , 6 , 7 , 8 , 9 ,
- Marc Suárez-Calvet ORCID: orcid.org/0000-0002-2993-569X 5 , 6 , 7 , 8 , 9 ,
- Sterling C. Johnson ORCID: orcid.org/0000-0002-8501-545X 10 ,
- Reisa Sperling ORCID: orcid.org/0000-0003-1535-6133 11 ,
- Alexandre Bejanin ORCID: orcid.org/0000-0002-9958-0951 1 , 2 ,
- Alberto Lleó ORCID: orcid.org/0000-0002-2568-5478 1 , 2 &
- Víctor Montal ORCID: orcid.org/0000-0002-5714-9282 1 , 2 , 12 na1
Nature Medicine ( 2024 ) Cite this article
11k Accesses
4199 Altmetric
Metrics details
- Alzheimer's disease
- Predictive markers
This study aimed to evaluate the impact of APOE4 homozygosity on Alzheimer’s disease (AD) by examining its clinical, pathological and biomarker changes to see whether APOE4 homozygotes constitute a distinct, genetically determined form of AD. Data from the National Alzheimer’s Coordinating Center and five large cohorts with AD biomarkers were analyzed. The analysis included 3,297 individuals for the pathological study and 10,039 for the clinical study. Findings revealed that almost all APOE4 homozygotes exhibited AD pathology and had significantly higher levels of AD biomarkers from age 55 compared to APOE3 homozygotes. By age 65, nearly all had abnormal amyloid levels in cerebrospinal fluid, and 75% had positive amyloid scans, with the prevalence of these markers increasing with age, indicating near-full penetrance of AD biology in APOE4 homozygotes. The age of symptom onset was earlier in APOE4 homozygotes at 65.1, with a narrower 95% prediction interval than APOE3 homozygotes. The predictability of symptom onset and the sequence of biomarker changes in APOE4 homozygotes mirrored those in autosomal dominant AD and Down syndrome. However, in the dementia stage, there were no differences in amyloid or tau positron emission tomography across haplotypes, despite earlier clinical and biomarker changes. The study concludes that APOE4 homozygotes represent a genetic form of AD, suggesting the need for individualized prevention strategies, clinical trials and treatments.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
195,33 € per year
only 16,28 € per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
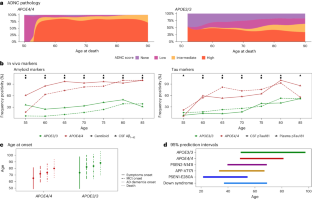
Similar content being viewed by others

Exceptionally low likelihood of Alzheimer’s dementia in APOE2 homozygotes from a 5,000-person neuropathological study

Association of APOE e2 genotype with Alzheimer’s and non-Alzheimer’s neurodegenerative pathologies

Apolipoprotein E and Alzheimer disease: pathobiology and targeting strategies
Data availability.
Access to tabular data from ADNI ( https://adni.loni.usc.edu/ ), OASIS ( https://oasis-brains.org/ ), A4 ( https://ida.loni.usc.edu/collaboration/access/appLicense.jsp ) and NACC ( https://naccdata.org/ ) can be requested online, as publicly available databases. All requests will be reviewed by each studyʼs scientific board. Concrete inquiries to access the WRAP ( https://wrap.wisc.edu/data-requests-2/ ) and ALFA + ( https://www.barcelonabeta.org/en/alfa-study/about-the-alfa-study ) cohort data can be directed to each study team for concept approval and feasibility consultation. Requests will be reviewed to verify whether the request is subject to any intellectual property.
Code availability
All statistical analyses and raw figures were generated using R (v.4.2.2). We used the open-sourced R packages of ggplot2 (v.3.4.3), dplyr (v.1.1.3), ggstream (v.0.1.0), ggpubr (v.0.6), ggstatsplot (v.0.12), Rmisc (v.1.5.1), survival (v.3.5), survminer (v.0.4.9), gtsummary (v.1.7), epitools (v.0.5) and statsExpression (v.1.5.1). Rscripts to replicate our findings can be found at https://gitlab.com/vmontalb/apoe4-asdad (ref. 32 ). For neuroimaging analyses, we used Free Surfer (v.6.0) and ANTs (v.2.4.0).
Bellenguez, C. et al. New insights into the genetic etiology of Alzheimer’s disease and related dementias. Nat. Genet. 54 , 412–436 (2022).
Article CAS PubMed PubMed Central Google Scholar
Frisoni, G. B. et al. The probabilistic model of Alzheimer disease: the amyloid hypothesis revised. Nat. Rev. Neurosci. 23 , 53–66 (2022).
Article CAS PubMed Google Scholar
Bateman R. J. et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 367 , 795–804 (2012).
Genin, E. et al. APOE and Alzheimer disease: a major gene with semidominant inheritance. Mol. Psychiatry 16 , 903–907 (2011).
Fortea, J. et al. Alzheimer’s disease associated with Down syndrome: a genetic form of dementia. Lancet Neurol. 20 , 930–942 (2021).
Fortea, J. et al. Clinical and biomarker changes of Alzheimer’s disease in adults with Down syndrome: a cross-sectional study. Lancet 395 , 1988–1997 (2020).
Jansen, W. J. et al. Prevalence of cerebral amyloid pathology in persons without dementia: a meta-analysis. JAMA 313 , 1924–1938 (2015).
Article PubMed PubMed Central Google Scholar
Saddiki H. et al. Age and the association between apolipoprotein E genotype and Alzheimer disease: a cerebrospinal fluid biomarker-based case-control study. PLoS Med. https://doi.org/10.1371/JOURNAL.PMED.1003289 (2020).
Jack, C. R. et al. NIA‐AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 14 , 535–562 (2018).
Article Google Scholar
Beekly, D. L. et al. The National Alzheimer’s Coordinating Center (NACC) Database: an Alzheimer disease database. Alzheimer Dis. Assoc. Disord. 18 , 270–277 (2004).
PubMed Google Scholar
Montine, T. J. et al. National Institute on Aging–Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease: a practical approach. Acta Neuropathol. 123 , 1–11 (2012).
Reiman, E. M. et al. Exceptionally low likelihood of Alzheimer’s dementia in APOE2 homozygotes from a 5,000-person neuropathological study. Nat. Commun. 11 , 1–11 (2020).
Iulita M. F. et al. Association of Alzheimer disease with life expectancy in people with Down syndrome. JAMA Netw. Open https://doi.org/10.1001/JAMANETWORKOPEN.2022.12910 (2022).
Corder, E. H. et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 261 , 921–923 (1993).
Fortea, J., Quiroz, Y. T. & Ryan, N. S. Lessons from Down syndrome and autosomal dominant Alzheimer’s disease. Lancet Neurol. 22 , 5–6 (2023).
Therriault, J. et al. Frequency of biologically defined Alzheimer’s disease in relation to age, sex, APOE ε4, and cognitive impairment. Neurology 96 , e975–e985 (2021).
Betthauser, T. J. et al. Multi-method investigation of factors influencing amyloid onset and impairment in three cohorts. Brain 145 , 4065–4079 (2022).
Snellman, A. et al. APOE ε4 gene dose effect on imaging and blood biomarkers of neuroinflammation and beta-amyloid in cognitively unimpaired elderly. Alzheimers Res. Ther. 15 , 71 (2023).
Ghisays, V. et al. Brain imaging measurements of fibrillar amyloid-β burden, paired helical filament tau burden, and atrophy in cognitively unimpaired persons with two, one, and no copies of the APOE ε4 allele. Alzheimers Dement. 16 , 598–609 (2020).
Mehta, R. I. & Schneider, J. A. What is ‘Alzheimer’s disease’? The neuropathological heterogeneity of clinically defined Alzheimer’s dementia. Curr. Opin. Neurol. 34 , 237–245 (2021).
van der Lee, S. J. et al. The effect of APOE and other common genetic variants on the onset of Alzheimer’s disease and dementia: a community-based cohort study. Lancet Neurol. 17 , 434–444 (2018).
Belloy, M. E., Napolioni, V. & Greicius, M. D. A quarter century of APOE and Alzheimera’s disease: progress to date and the path forward. Neuron 101 , 820–838 (2019).
Belloy, M. E. et al. APOE genotype and Alzheimer disease risk across age, sex, and population ancestry. JAMA Neurol. 80 , 1284–1294 (2023).
Jack, C. R. et al. Long-term associations between amyloid positron emission tomography, sex, apolipoprotein E and incident dementia and mortality among individuals without dementia: hazard ratios and absolute risk. Brain Commun. 4 , fcac017 (2022).
Morris, J. C. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 43 , 2412–2414 (1993).
Weiner, M. W. et al. The Alzheimer’s Disease Neuroimaging Initiative 3: continued innovation for clinical trial improvement. Alzheimer’s Dement. 13 , 561–571 (2017).
Sperling R. A. et al. The A4 Study: stopping AD before symptoms begin? Sci. Transl. Med. https://doi.org/10.1126/scitranslmed.3007941 (2014).
Molinuevo, J. L. et al. The ALFA project: a research platform to identify early pathophysiological features of Alzheimer’s disease. Alzheimer’s Dement.: Transl. Res. Clin. Interventions 2 , 82–92 (2016).
Johnson, S. C. et al. The Wisconsin Registry for Alzheimer’s Prevention: a review of findings and current directions. Alzheimer’s Dement.: Diagnosis, Assess. Dis. Monit. 10 , 130–142 (2018).
Google Scholar
LaMontagne P. J. et al. OASIS-3: longitudinal neuroimaging, clinical and cognitive dataset for normal aging and Alzheimer disease. Preprint at MedRxiv https://doi.org/10.1101/2019.12.13.19014902 (2019).
La Joie, R. et al. Multisite study of the relationships between antemortem [ 11 C]PIB-PET Centiloid values and postmortem measures of Alzheimer’s disease neuropathology. Alzheimers Dement. 15 , 205–216 (2019).
Montal, V. APOE4-ASDAD. GitLab https://gitlab.com/vmontalb/apoe4-asdad (2024).
Download references
Acknowledgements
We acknowledge the contributions of several consortia that provided data for this study. We extend our appreciation to the NACC, the Alzheimer’s Disease Neuroimaging Initiative, The A4 Study, the ALFA Study, the Wisconsin Register for Alzheimer’s Prevention and the OASIS3 Project. Without their dedication to advancing Alzheimer’s disease research and their commitment to data sharing, this study would not have been possible. We also thank all the participants and investigators involved in these consortia for their tireless efforts and invaluable contributions to the field. We also thank the institutions that funded this study, the Fondo de Investigaciones Sanitario, Carlos III Health Institute, the Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas and the Generalitat de Catalunya and La Caixa Foundation, as well as the NIH, Horizon 2020 and the Alzheimer’s Association, which was crucial for this research. Funding: National Institute on Aging. This study was supported by the Fondo de Investigaciones Sanitario, Carlos III Health Institute (INT21/00073, PI20/01473 and PI23/01786 to J.F., CP20/00038, PI22/00307 to A.B., PI22/00456 to M.S.-C., PI18/00435 to D.A., PI20/01330 to A.L.) and the Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas Program 1, partly jointly funded by Fondo Europeo de Desarrollo Regional, Unión Europea, Una Manera de Hacer Europa. This work was also supported by the National Institutes of Health grants (R01 AG056850; R21 AG056974, R01 AG061566, R01 AG081394 and R61AG066543 to J.F., S10 OD025245, P30 AG062715, U54 HD090256, UL1 TR002373, P01 AG036694 and P50 AG005134 to R.S.; R01 AG027161, R01 AG021155, R01 AG037639, R01 AG054059; P50 AG033514 and P30 AG062715 to S.J.) and ADNI (U01 AG024904), the Department de Salut de la Generalitat de Catalunya, Pla Estratègic de Recerca I Innovació en Salut (SLT006/17/00119 to J.F.; SLT002/16/00408 to A.L.) and the A4 Study (R01 AG063689, U24 AG057437 to R.A.S). It was also supported by Fundación Tatiana Pérez de Guzmán el Bueno (IIBSP-DOW-2020-151 o J.F.) and Horizon 2020–Research and Innovation Framework Programme from the European Union (H2020-SC1-BHC-2018-2020 to J.F.; 948677 and 847648 to M.S.-C.). La Caixa Foundation (LCF/PR/GN17/50300004 to M.S.-C.) and EIT Digital (Grant 2021 to J.D.G.) also supported this work. The Alzheimer Association also participated in the funding of this work (AARG-22-923680 to A.B.) and A4/LEARN Study AA15-338729 to R.A.S.). O.D.-I. receives funding from the Alzheimer’s Association (AARF-22-924456) and the Jerome Lejeune Foundation postdoctoral fellowship.
Author information
These authors contributed equally: Juan Fortea, Víctor Montal.
Authors and Affiliations
Sant Pau Memory Unit, Hospital de la Santa Creu i Sant Pau - Biomedical Research Institute Sant Pau, Barcelona, Spain
Juan Fortea, Jordi Pegueroles, Daniel Alcolea, Olivia Belbin, Oriol Dols-Icardo, Lídia Vaqué-Alcázar, Laura Videla, Alexandre Bejanin, Alberto Lleó & Víctor Montal
Centro de Investigación Biomédica en Red de Enfermedades Neurodegenerativas. CIBERNED, Barcelona, Spain
Juan Fortea, Jordi Pegueroles, Daniel Alcolea, Olivia Belbin, Oriol Dols-Icardo, Laura Videla, Alexandre Bejanin, Alberto Lleó & Víctor Montal
Barcelona Down Medical Center, Fundació Catalana Síndrome de Down, Barcelona, Spain
Juan Fortea & Laura Videla
Department of Medicine, Faculty of Medicine and Health Sciences, Institute of Neurosciences, University of Barcelona, Barcelona, Spain
Lídia Vaqué-Alcázar
Barcelonaβeta Brain Research Center (BBRC), Pasqual Maragall Foundation, Barcelona, Spain
Juan Domingo Gispert & Marc Suárez-Calvet
Neurosciences Programme, IMIM - Hospital del Mar Medical Research Institute, Barcelona, Spain
Department of Medicine and Life Sciences, Universitat Pompeu Fabra, Barcelona, Spain
Centro de Investigación Biomédica en Red Bioingeniería, Biomateriales y Nanomedicina. Instituto de Salud carlos III, Madrid, Spain
Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain
Wisconsin Alzheimer’s Disease Research Center, University of Wisconsin-Madison School of Medicine and Public Health, Madison, WI, USA
Sterling C. Johnson
Brigham and Women’s Hospital Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
Reisa Sperling
Barcelona Supercomputing Center, Barcelona, Spain
Víctor Montal
You can also search for this author in PubMed Google Scholar
Contributions
J.F. and V.M. conceptualized the research project and drafted the initial manuscript. V.M., J.P. and J.F. conducted data analysis, interpreted statistical findings and created visual representations of the data. O.B. and O.D.-I. provided valuable insights into the genetics of APOE. L.V., A.B. and L.V.-A. meticulously reviewed and edited the manuscript for clarity, accuracy and coherence. J.D.G., M.S.-C., S.J. and R.S. played pivotal roles in data acquisition and securing funding. A.L. and D.A. contributed to the study design, offering guidance and feedback on statistical analyses, and provided critical review of the paper. All authors carefully reviewed the manuscript, offering pertinent feedback that enhanced the study’s quality, and ultimately approved the final version.
Corresponding authors
Correspondence to Juan Fortea or Víctor Montal .
Ethics declarations
Competing interests.
S.C.J. has served at scientific advisory boards for ALZPath, Enigma and Roche Diagnostics. M.S.-C. has given lectures in symposia sponsored by Almirall, Eli Lilly, Novo Nordisk, Roche Diagnostics and Roche Farma, received consultancy fees (paid to the institution) from Roche Diagnostics and served on advisory boards of Roche Diagnostics and Grifols. He was granted a project and is a site investigator of a clinical trial (funded to the institution) by Roche Diagnostics. In-kind support for research (to the institution) was received from ADx Neurosciences, Alamar Biosciences, Avid Radiopharmaceuticals, Eli Lilly, Fujirebio, Janssen Research & Development and Roche Diagnostics. J.D.G. has served as consultant for Roche Diagnostics, receives research funding from Hoffmann–La Roche, Roche Diagnostics and GE Healthcare, has given lectures in symposia sponsored by Biogen, Philips Nederlands, Esteve and Life Molecular Imaging and serves on an advisory board for Prothena Biosciences. R.S. has received personal consulting fees from Abbvie, AC Immune, Acumen, Alector, Bristol Myers Squibb, Janssen, Genentech, Ionis and Vaxxinity outside the submitted work. O.B. reported receiving personal fees from Adx NeuroSciences outside the submitted work. D.A. reported receiving personal fees for advisory board services and/or speaker honoraria from Fujirebio-Europe, Roche, Nutricia, Krka Farmacéutica and Esteve, outside the submitted work. A.L. has served as a consultant or on advisory boards for Almirall, Fujirebio-Europe, Grifols, Eisai, Lilly, Novartis, Roche, Biogen and Nutricia, outside the submitted work. J.F. reported receiving personal fees for service on the advisory boards, adjudication committees or speaker honoraria from AC Immune, Adamed, Alzheon, Biogen, Eisai, Esteve, Fujirebio, Ionis, Laboratorios Carnot, Life Molecular Imaging, Lilly, Lundbeck, Perha, Roche and outside the submitted work. O.B., D.A., A.L. and J.F. report holding a patent for markers of synaptopathy in neurodegenerative disease (licensed to Adx, EPI8382175.0). The remaining authors declare no competing interests.
Peer review
Peer review information.
Nature Medicine thanks Naoyuki Sato, Yadong Huang and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Jerome Staal, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information.
Supplementary Methods, Results, Bibliography, Figs. 1–7 and Tables 1–3.
Reporting Summary
Supplementary code.
This code is also available in the GitLab repository.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Fortea, J., Pegueroles, J., Alcolea, D. et al. APOE4 homozygozity represents a distinct genetic form of Alzheimer’s disease. Nat Med (2024). https://doi.org/10.1038/s41591-024-02931-w
Download citation
Received : 03 November 2023
Accepted : 19 March 2024
Published : 06 May 2024
DOI : https://doi.org/10.1038/s41591-024-02931-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

GLOBAL Raises $400,000 at their AcceptAbility Gala as Celebrities & Congress Step Out for People with Down Syndrome
Washington, DC, May 10, 2024 (GLOBE NEWSWIRE) — Last night the Global Down Syndrome Foundation (GLOBAL) held its sixth annual AcceptAbility Gala , DC’s largest fundraiser for people with Down syndrome, that raised $400,000 to support important research and medical care to improve the lives of those who happen to have Down syndrome. Representatives Richard Hudson (R-NC) and Lois Frankel (D-FL) received GLOBAL’s highest honor, the Quincy Jones Exceptional Advocacy Award, and pledged their continued strong advocacy in Congress that makes an impact on the lives of people with Down syndrome and their families.
“At GLOBAL, we are working hard every day to elongate life and improve health outcomes for our loved ones with Down syndrome,” says GLOBAL Co-Founder, President, and CEO, Michelle Sie Whitten . “Last night we brought together a room full of bi-partisan support from Congress, NIH leadership, self-advocates with Down syndrome, and corporate leaders, all celebrating the impact of GLOBAL’s work. The joy and excitement at our event and the tangible outcome of our work together is truly rewarding!”
Held at the Marriott Marquis in Washington, DC, the event was attended by GLOBAL awardee alum, Representative Cathy McMorris Rodgers (R-WA) and her son, GLOBAL Ambassador Cole Rodgers . Representative Rodgers’ keynote speech deeply moved the audience. Her determination to pass a game-changing legacy bill, the DeOndra Dixon INCLUDE Project Act, before her poignant retirement from Congress was an important feature of the evening. The bill will help ensure funding for Down syndrome research and medical care from the NIH for years to come.
Celebrities passionate about the cause included Grammy-nominated, multi-platinum singer/songwriter and actress Jordin Sparks ; actor, author and public speaker Frank Stephens ; author and public speaker David Egan ; and award-winning correspondent for ABC News and anchor for ABC News LIVE Kyra Phillips and her daughter Sage Roberts.
To recognize the transformative leadership of Representative Rosa DeLauro (D-CT), the GLOBAL Rosa DeLauro Advancement Award, with a post-secondary scholarship, was provided to Damani Tichawonna from Washington, DC as was the GLOBAL Tom Cole Advancement Award to Julia Greene . Representative Rosa DeLauro was on-hand to personally present both Advancement Awards to the deserving recipients, leaving the audience inspired to do even more for people with Down syndrome and their families.
With the help of GLOBAL Ambassador Isla Eager and her family, Erin Book Mullen , and co-chairs Julie Riccio and Amy Best Weiss , the inspirational gala attracted 300 attendees and raised $400,000 for GLOBAL’s life-saving research and medical care. GLOBAL supports over 200 researchers on the Anschutz Medical Campus at the Crnic Institute for Down Syndrome and at the Alzheimer’s and Cognition Center, as well as 2,500 patients from 33 states and 10 countries at the Sie Center for Down Syndrome. For nearly two decades, Down syndrome was one of the least federally funded genetic conditions in the United States.
“People with Down syndrome enrich our world in unique ways,” says Representative Hudson. “GLOBAL is paving the way for people who are differently-abled so they can live their lives to their full potential with no barriers or bias or obstacles standing in their way. I am honored to support their efforts and to receive this award, and will continue advocating for policies that improve the lives of people with Down syndrome.”
“It was an honor to be with so many great advocates for Down syndrome and to receive such a generous recognition,” says Representative Frankel. “I am proud to support GLOBAL’s mission of elongating life and improving health outcomes for people with Down syndrome. Their AcceptAbility Gala was an inspiring evening that reminds all of us that we must continue to make critical investments in Down syndrome research to uphold the health and dignity of every person.”
At the end of the evening, Jordin Sparks wowed the audience not only with her beautiful voice but by connecting with fans and bringing self-advocates with Down syndrome on stage while performing an intimate, heartfelt performance of some of her biggest hits including “No Air” and “One Step at a Time,” and solo dancer Robert Wallop and inclusive dance troupe RhythmXpress delighted attendees with dance performances set to “Bones” by Imagine Dragons, “Firework” by Katy Perry and “Fireball” by Mini Pop Kids.
Additional notables in attendance included Kim Owens from the National Down Syndrome Congress and Dria Law from the Down Syndrome Association of Southern New Jersey .
To learn more about GLOBAL, visit www.globaldownsyndrome.org.
About the Global Down Syndrome Foundation
The Global Down Syndrome Foundation (GLOBAL) is the largest non-profit in the U.S. working to save lives and dramatically improve health outcomes for people with Down syndrome. GLOBAL has donated more than $32 million to establish the first Down syndrome research institute supporting over 400 scientists and over 2,400 patients with Down syndrome from 33 states and 10 countries. Working closely with Congress and the National Institutes of Health, GLOBAL is the lead advocacy organization in the U.S. for Down syndrome research and medical care. GLOBAL has a membership of over 110 Down syndrome organizations worldwide and is part of a network of Affiliates – the Crnic Institute for Down Syndrome, the Sie Center for Down Syndrome, and the University of Colorado Alzheimer’s and Cognition Center – all on the Anschutz Medical Campus. GLOBAL’s widely circulated medical publications include GLOBAL Medical Care Guidelines for Adults with Down Syndrome, Prenatal & Newborn Down Syndrome Information, and the award-winning Down Syndrome World™ magazine. GLOBAL also organizes the annual AcceptAbility Gala in Washington DC, and the annual Be Beautiful Be Yourself Fashion Show , the largest Down syndrome fundraiser in the world.
Attachments
- GLOBAL's Quincy Jones Exceptional Advocacy Awardees
- 2024 AcceptAbility Gala Performer Jordin Sparks
Shawn Flaherty
Global Down Syndrome Foundation
703-554-3609
COMMENTS
Down syndrome (DS) is a birth defect with huge medical and social costs, caused by trisomy of whole or part of chromosome 21. It is the most prevalent genetic disease worldwide and the common genetic cause of intellectual disabilities appearing in about 1 in 400-1500 newborns. Although the syndrome had been described thousands of years before ...
Seborrheic dermatitis may occur in up to 30% of persons. with Down syndrome (general population 2-5%), with red. cheeks being common. With time, the skin has a tendency to. become dry and rough ...
Down's syndrome is the most common autosomal abnormality worldwide, affecting around 1 in 1000 live births (World Health Organization, 2018).In 2011, it was estimated that there were 37 000 people with the condition in England and Wales, with a population prevalence of 0.66 per 1000 (Wu and Morris, 2013).Down's syndrome accounts for one-third of cases of severe learning disability.
Down syndrome (DS) is one of the commonest disorders with huge medical and social cost. DS is associated with number of phenotypes including congenital heart defects, leukemia, Alzeihmer's disease, Hirschsprung disease etc. DS individuals are affected by these phenotypes to a variable extent thus understanding the cause of this variation is a key challenge. In the present review article, we ...
Down syndrome is a chromosomal disorder resulting from the existence of an extra copy chromosome 21. The condition got its name from John Land Down; the doctor who first described it. Down syndrome is associated with symptoms that impair cognitive ability, physical development and often alter facial appearance. We will write a custom essay on ...
Individuals with Down syndrome have seen improvements in quality of life and life expectancy in recent decades due to health-care and research advancements, along with greater societal participation. However, there are persistent disparities in health outcomes stemming from insufficient awareness and training about Down syndrome among physicians, professionals, families, and other stakeholders ...
Down syndrome (DS) is a form of accelerated aging, and people with DS are highly prone to aging-related conditions that include vascular and neurological disorders. Due to the overexpression of several genes on Chromosome 21, for example genes encoding amyloid precursor protein (APP), superoxide dismutase (SOD), and some of the interferon receptors, those with DS exhibit significant ...
This thesis will focus on children with Down syndrome. Down syndrome is a chromosomal disorder and one of the most common causes of intellectual disability (Carr, 1995). People with Down syndrome have distinctive facial features, which make them immediately identifiable to others and may mean that people with Down syndrome identify
Provocative new findings suggest a surprising cause of Down syndrome: cells linked to aging. Neural progenitor cells derived from stem cells of a person with Down syndrome. Courtesy Hiruy Meharena ...
Down Syndrome Research and Practice. Down Syndrome Research and Practice is a peer-reviewed journal focused on Down syndrome research. It was published by Down Syndrome Education International in partnership with the University of Portsmouth from 1992 to 2009. Volume 1. Issue 1.
Essay Title 3: Advances in Down Syndrome Research: Genetics, Therapies, and Future Prospects Thesis Statement: This essay delves into the realm of Down syndrome research, highlighting recent developments in genetics, therapeutic approaches, and the potential future directions that hold promise for improving the quality of life for individuals ...
Using current research literature on behavioral issues and novel treatments for Down syndrome, this paper explores and discusses behavioral inflexibility, restrictive and repetitive behaviors, and Down syndrome's neurogenetic nature. Down Syndrome: Prenatal Testing, Chronic Health Conditions, and Cognitive Deficits.
Overall, the analysis presents an everyday practice aimed at a desirable future for the child with Down syndrome and at a management of everyday life on the family's own terms. In conclusion, this study provides specific knowledge on parents' everyday practice, which may inform genetic counseling about Down syndrome and be of value to service ...
DSE hosts the annual Down Syndrome Research Forum, bringing researchers, students, practitioners and families together to discuss current research and practice. The Down Syndrome Research Forum 2024 was held on 25 and 26 April. We expect to announce the dates for the Down Syndrome Research Forum 2025 soon. Learn more. DSE Online.
The epidemiological profile as of 2010 investigations reveals that Down syndrome occurs at a rate of 1 in every 1000 birth globally accounting for an estimated 17,000 deaths annually. Pregnancies occurring at age 40 have a 1 in 84 chance of being Down syndrome. While the incidence of Down syndrome increases with age there is a 30% occurrence ...
Research Paper On Down Syndrome. They used to be called "Mongoloids," an ethnic insult coined by John Langdon Down, an English physician during the nineteenth century. But now they are known as people, individuals with a condition known as Down syndrome. (3). It wasn't until the 1960s that Jerome Lejeune and Patricia Jacobs discovered the cause ...
Introduction. Down syndrome (DS) is the most common neurodevelopmental disorder with known genetic causes, and an incidence of 1 in 691 live births ().This suggests that ~417,000 people with DS live in Europe ().Currently, an expansive menu of prenatal diagnostic methods for DS is spreading worldwide, advancing the diagnosis of DS from postnatal to prenatal ().
Vanderbilt University is committed to the principle of equal opportunity. Vanderbilt University does not discriminate against individuals on the basis of their race, sex, sexual orientation, gender identity, religion, color, national or ethnic origin, age, disability, military service, or genetic information in its administration of educational policies, programs, or activities; admissions ...
We would like to note that Down syndrome underwent a similar recent reappraisal 5 based on the demonstration of universal AD pathology, the predictable sequence of biomarkers and clinical changes ...
GLOBAL has donated more than $32 million to establish the first Down syndrome research institute supporting over 400 scientists and over 2,400 patients with Down syndrome from 33 states and 10 ...
GLOBAL has donated more than $32 million to establish the first Down syndrome research institute supporting over 400 scientists and over 2,400 patients with Down syndrome from 33 states and 10 countries. Working closely with Congress and the National Institutes of Health, GLOBAL is the lead advocacy organization in the U.S. for Down syndrome ...